Blount Disease
Farzad Pourghazi1, Sammy Mohammadi1, Philippe Violas2, Maysa Eslami1, Mohammad Hossein Nabian1*
1Center for Orthopedic Trans-disciplinary Applied Research (COTAR) Tehran University of Medical Science, Iran.
2Professor, Pediatric Orthopedic Service, Central Hospital University of Rennes, 35000 Rennes, France.
*Corresponding Author:Mohammad Hossein Nabian, Jalal-Al-Ahmad Street, North Kargar Avenue, Shariati Hospital, Tehran, Iran, Center for Orthopedic Trans-disciplinary Applied Research (COTAR) Tehran University of Medical Science,Iran, Tel+989126305095; Fax: +989126305095; E-mail:dr.nabian@gmail.com
Citation: Mohammad Hossein Nabian, Farzad Pourghazi, Sammy Mohammadi, Philippe Violas, Maysa Eslami, et al. (2022) Blount Disease. Pediatr Primary Physic 2: 113.
Received: December 22, 2022; Accepted: December 25, 2022; Published: January 05,2023
Copyright: © 2022Mohammad Hossein Nabian, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background
Blount disease is an acquired growth disorder of medial proximal tibial physis and epiphysis; this disease causes the medial growth plate of the proximal tibia to slow down or stop the growth while the lateral physis of the proximal tibia grow normally. Thus, this change leads to varus malalignments [1,2]. Blount first described Blount disease in [3,4]. There are two types of Blount disease. The first one starts at the early age of life (Earlier than 10 years old), which we call the infantile type, and the second type starts after 10 years of age, which we call the adolescent type. Obese individuals, African-Americans and early walkers are at the greater risk of developing Blount disease [5]. Blount disease is been reported bilateral in approximately 50 percent of patients afflicted with this disorder [5].
In the history-taking process, early walking is common, before one year of age. Bowed knees also can be found in normal infants, especially until one year after they begin to walk. However, the varus deformity in normal infants is symmetrical, and the knee is stable. Persistent genu varum in the obese child is the first clue for the physician to diagnose Blount disease [1].
Lateral thrust during weight bearing is another key finding [6].In most cases, irreversible knee changes, especially after 6 to 8 years old, lead to poor response to conservative treatment. Especially in African-Americans, Blount disease worsens through time until walking is impossible for the patients. In adults, Osteoarthritis develops prematurely between 30 to 50 years of age [1,5,6]. According to Leville et al., one-third of patients heal spontaneously [7]. Another study in Japan showed spontaneous healing of the disease in 22 cases [8].If the infantile type is treated at early stages prognosis is not that poor, and the recurrence of the disease is rare; without therapy, on the opposite side, infantile Blount disease has progressive characteristics [9].
Inaccurate treatment of Blount disease leads to persistent pain, decreased school function, low self-esteem, and depression [10,11]. In conclusion, knowing the appropriate treatment and early diagnosis of Blount disease is very important in the future outcomes of patients.
Keywords
Keywords: Blount Disease, Radiography, Osteotomy
Step1: Which imaging studies do we need for the diagnosis of Blount disease?
Regardless of the patient’s age, presence of a lateral thrust of the knee is an indication for radiographs, even if it is not pathognomonic for infantile tibia vara [12].In addition to diagnosing Blount disease, radiographs help us rule out other diseases.
Anterio-Posterior view of both Knees (AP radiography) and Lateral view of both knees:
Standing AP x-ray of both knees in the early stages of Blount disease helps us to see varus malalignment of the proximal tibia. Delayed medial proximal tibial physis growth leads to the epiphyseal slope. Thus, this irregularity of the medial tibia causes lateral tibial subluxation in some cases (1). Hence, Prominent beaking of the medial metaphysis with lucent cartilage islands within the beak may be detectable.Figure 1 shows AP xray of a child with Blount disease.
Figure 1: Tibia vara in a Female child with Blount disease. AP x ray. (A=15?) proximal metaphyseal-diaphyseal angle. (B) the beak of the medial metaphysis (13).

This view shows both legs from hip to ankles, and we can see Varus deformity of the knee in this radiograph, especially in the early stages of Blount disease [1]. Figure 2 shows long leg AP radiograph of a patient with Blount disease.
Figure 2: 2 years old male with diagnosis of Blount disease. Long leg AP radiograph (3-joint view) [14]. (A=22.5?) Tibiofemoral angle.
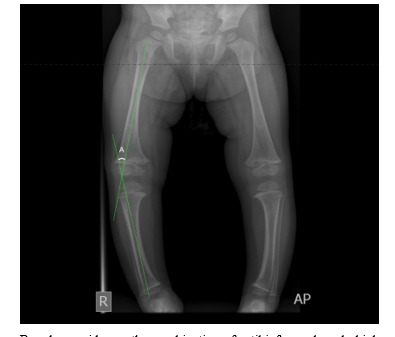
Based on evidence, the combination of a tibiofemoral angle higher than 20 degrees with an MDA (metaphyseal-diaphyseal angle) more than 10 degrees indicates a toddler at risk of the blount disease [15].
Magnetic Resonance Imaging (MRI)
In addition to a better image of soft tissues such as cartilage, meniscus, and ligaments, MRI with the injection of gadolinium provides images of blood supply to the growth plates [16,17]. Figure 3 shows an MRI (T1) imaging of a patient with Blount disease. MRI is not necessary to confirm the diagnosis, but it is a useful prospective tool for characterizing the extent of the ossified and cartilaginous epiphysis along with any physeal anatomic defect [12].
Figure 3: MRI imaging (T1). Patient with Blount disease (18).

Step2: What should we focus on in radiographs for better diagnosis?
Metaphysical diaphyseal angle (MDA) (Drennan)
This angle is defined as a line connecting metaphyseal beaks and a line perpendicular to the longitudinal axis of the tibia.
MDA value Greater than 16° is considered abnormal, and patients who developed this degree of more than 16° have a 95% chance of disease progression. We should observe patients closely if the angle was between 11-16°. MDA<10° has a 95% chance of spontaneously healing [5,19]. Patient in Figure1 shows 15-degree angle of Drennan on both sides.
Bony Tibial Slope
Step 3: Follow-up of symptomatic, progressive patients
Progressive, symptomatic patients should be followed up at least every 6 months. Follow-up should start at ages between 4 to 5 years. Follow-up is evaluated by clinical examination and measurements of MDA angle by radiographs.
Step 4: What kind of treatments should we consider for infantile Blount disease?
The treatment approach is guided mainly by the radiographic findings and patient’s age. Considering metaphyseal-epiphyseal changes seen on radiographs, Langenskiöld suggested a classification for infantile tibia vara varying with advancing age in 1952, which is being used until today [4]. It contains six progressive stages which is shown in Figure 5.
Non-operative management (Orthoses)
Braces for non-operative treatment should be used for children younger than 3 years old with early Langenskiöld stage I to II lesions; however, in most cases, the osteotomy is indicated before four years of age. Blount disease braces generally extend from the upper part of the thigh until the foot; These braces apply valgus force to the knee to improve deformity. However, the use of braces is deputed according to various reports [20]. Different sort of braces has been utilized over time for blount disease, but the elastic KAFOs (knee-ankle-foot orthosis) are used exclusively nowadays due to ease of fabrication and smaller profile. The elastic blount brace has a medial upright design and contains wide elastic band distal to the knee joint [21].
Figure 4: Elastic blount brace [22].

Surgical Treatment
In severe Blount disease cases, surgical axis re-alignments should be performed before age 4. If patients surgically be treated before the age of four, they will recover in 80% of cases. Lateral thrust is a key finding for the diagnosis of knee failure [1,6]. Surgical choices are different; We should choose them according to the severity of symptoms and the age of onset. Surgical techniques include:
Graded Growth
Lateral plate growth inhibition with staples, pin, and tension band plating is a commonly used procedure. However, published studies are small, and they have various designs. Lateral plate growth inhibition techniques can correct the varus deformity, but these techniques can not correct the rotational component of the deformity. These techniques are not appropriate for obese patients [2,6].
Osteotomy Procedures
Surgical technique should be personalized by the severity of the disease, age, differences in limb length, and surgeon's experience. Our goal for the treatment of Blount disease is to achieve a stable and correct oriented lower extremity [23]. Proximal tibial osteotomy (PTO) or high tibial osteotomy is a proven technique in treating Blount disease [24]. Even in severe cases, Blount disease could be treated in most of the cases by proximal tibial osteotomy [25]. Several surgery techniques were developed for deformity correction in Blount diseases, such as open-wedge, close-wedge, oblique, and dome osteotomies.
Open and Close Wedge Osteotomy
Opening-closing wedge osteotomy is proven a safe and effective technique for treating Blount disease [26].The closing wedge may cause additional leg shortening [27,28]. On the other hand, closing-wedge osteotomy, despite the open-wedge, does not need an iliac crest graft [28]. Open wedge osteotomy does not correct rotational deformity and leg length discrepancy [29]. Also, open-wedge osteotomy may cause under-correction of internal tibial torsion. In this case we have to do rigid internal fixation [27].
Dome Osteotomy
A study by Musikachart et al. showed no significant difference between the outcomes of wedge-shaped osteotomies and dome osteotomies. They showed similar results in repetitive long-term follow-up [11].
Oblique osteotomy
In this procedure rapid union of two bone fragments simultaneously remodeled deformities, but this type of procedure is not an appropriate option if there is a) medial condyle depression and b) leg-length discrepancy [30].
Inverted V-shaped PTO and other techniques
Inverted V-shaped PTO would be considered one of the effective and safe treatments for severely obese, young, and highly active patients (31, 32). Some of these personalized experimental procedures are useful; They provide enough correction (32, 33). They require smaller resection and opening compared to opening-closing osteotomies. They also preserve patellar height despite wedge-osteotomies [28,32,33].
Step 5: Post-operative correction techniques
There are various postoperative fixation techniques to help with correction and healing. These techniques include calcified cast immobilization, K-Wires, staples, screws, Ilizarov, etc. [10,33].
Summary
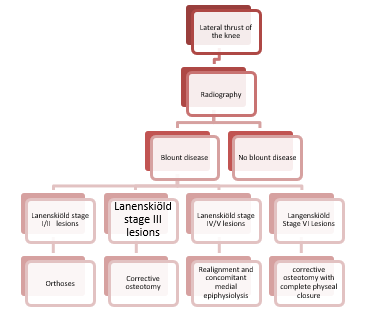
In conclusion, early diagnosis of Blount disease is very important due to the long-term consequences of late diagnosis. Treatments should be considered from early ages; conservative treatments such as braces should be considered before three years of age. However, most cases need early surgery for correct deformity. Every orthopedic surgeon should be completely aware of the management of Blount disease. Figure 6 shows summary of Blount disease Management [12].
Figure 5: Langenskiöld classification.
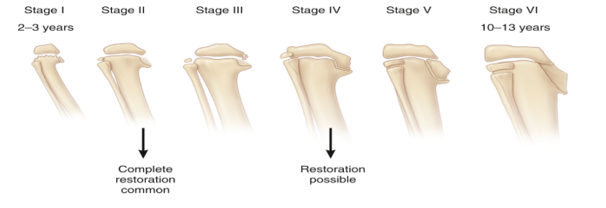
Figure 6: Algorithm for blount disease management.
References
- Janoyer M (2019) Blount disease. Orthopaedics & Traumatology: Surgery & Research.105: S111-S21.
- Sabharwal S (2009) Blount disease. JBJS 91: 1758-76.
- Blount W (1937) Tibia vara: osteochondrosis deformans tibiae. JBJS 19: 1-29.
- Langenskiöld A, Riska EB (1964) Tibia vara (osteochondrosis deformans tibiae): a survey of seventy-one cases. JBJS 46:1405-1420.
- De Leucio A (2021) Blount Disease. StatPearls [Internet]: StatPearls Publishing.
- Herring J, Genu varum (2002) Tachdjian's pediatric orthopedics 3rd ed Philadelphia: Saunders 839-855.
- Laville J-M, Wiart Y, Salmeron F (2010) Can Blount's disease heal spontaneously? Orthopaedics & Traumatology: Surgery & Research 96: 531-535.
- Shinohara Y, Kamegaya M, Kuniyoshi K, Moriya H (2002) Natural history of infantile tibia vara. The Journal of bone and joint surgery British volume 84: 263-268.
- Doyle BS, Volk AG, Smith CF (1996) Infantile Blount disease: long-term follow-up of surgically treated patients at skeletal maturity. J Pediatr Orthop 16: 469-476.
- Ghasemi SA, Zhang DT, Fragomen A, Rozbruch SR (2021) Proximal tibial osteotomy for genu varum: Radiological evaluation of deformity correction with a plate vs external fixator. World Journal of Orthopedics 12: 140.
- Musikachart P, Eamsobhana P (2020) Do Different Tibial Osteotomy Techniques Affect Sagittal Alignment in Children with Blount Disease? Orthopaedic Surgery 12: 770-775.
- Herring JA (2020) Tachdjian's Pediatric Orthopaedics: From the Texas Scottish Rite Hospital for Children E-Book: Elsevier Health Sciences
- AJ Jahangiri A, Blount disease. Case study, Radiopaedia.org
- HH Hamidi H, Blount disease. Case study, Radiopaedia.org
- Davids JR, Blackhurst DW, Allen Jr BL (2001) Radiographic evaluation of bowed legs in children. Journal of Pediatric Orthopaedics. 21: 257-263.
- Ho-Fung V, Jaimes C, Delgado J, Davidson RS, Jaramillo D, et al. (2013) MRI evaluation of the knee in children with infantile Blount disease: tibial and extra-tibial findings. Pediatric radiology 43: 1316-1326.
- Sabharwal S, Wenokor C, Mehta A, Zhao C (2012) Intra-articular morphology of the knee joint in children with Blount disease: a case-control study using MRI. JBJS 94: 883-890.
- Haouimi A BdCs, Radiopaedia.org (Accessed on 20 Dec 2022) Haouimi A, Blount disease. Case study, Radiopaedia.org
- Levine AM, Drennan JC (1982) Physiological bowing and tibia vara. The metaphyseal-diaphyseal angle in the measurement of bowleg deformities. The Journal of bone and joint surgery American volume 64: 1158-1163.
- Sabharwal S, Sabharwal S (2017) Treatment of Infantile Blount Disease: An Update. J Pediatr Orthop 37 Suppl 2: S26-s31.
- Supan TJ, Mazur J (1985) Orthotic correction of Blount’s disease. Clinical Orthotics and Prosthetics. 9: 3-6.
- Alsancak S, Guner S, K?n?k H (2020) improved Gait parameters After orthotic treatment in children with infantile tibia Vara. Scientific Reports 10: 1-7.
- Miraj F, Karda IWAM (2019) Step cut “V” osteotomy for acute correction in Blount’s disease treatment: A case series. International Journal of Surgery Case Reports 58: 57-62.
- Sananta P, Santoso J, Sugiarto MA (2022) Osteotomy treatments and post-operative fixations for Blount disease: A systematic review. Annals of Medicine and Surgery 103784.
- Abraham E, Toby D, Welborn M, Helder CW, Murphy A, et al. (2019) New single-stage double osteotomy for late-presenting infantile tibia vara: a comprehensive approach. Journal of pediatric orthopedics 39: 247.
- Obiegbu H (2021) Outcome of opening-closing wedge osteotomy in the correction of Blount’s disease. East African Orthopaedic Journal 15: 79-83.
- Karuppal R, Mohan R, Marthya A, Gopakumar T, Sandhya S, et al. (2015) Case Report: ‘Z’osteotomy-a novel technique of treatment in Blount’s disease 4.
- 28.Nada AA, Hammad ME, Eltanahy AF, Gazar AA, Khalifa AM, et al. (2021) Acute Correction and Plate Fixation for the Management of Severe Infantile Blount's Disease: Short-term Results. Strategies in Trauma and Limb Reconstruction 16: 78.
- Griswold B, Gilbert S, Khoury J (2018) Opening wedge osteotomy for the correction of adolescent tibia vara. The Iowa Orthopaedic Journal 38: 141.
- Aly AS, Abdelhamid Alsabir AR, Fahmy HA, Fayyad TA (2021) Modified oblique high tibial osteotomy with minimal fixation for correction of adolescent tibia vara: a prospective case series study. Journal of Children's Orthopaedics 15: 6-11.
- Hayashi S, Tsukisaka K, Aoki T, Okuhara A (2021) Inversed V-shaped High Tibial Osteotomy for Severe Varus Deformity due to Blount Disease: A Case Report. Journal of Orthopaedic Case Reports11: 29.
- Abe D, Hamai S, Okazaki K, Yoshimoto M, Komatsu T, et al. (2018) Inverted V-shaped high tibial osteotomy for severe tibia vara associated with Turner syndrome: A case report and review of literature. International journal of surgery case reports 42: 128-132.
- Baraka MM, Hefny HM, Mahran MA, Fayyad TA, Abdelazim H et al., Single-stage medial plateau elevation and metaphyseal osteotomies in advanced-stage Blount's disease: A new technique.