Circulating Tumor Cells - The Future of Medicine as Diagnostic and Therapeutic Biomarker”
Ajit Kumar Saxena1*
1Human Molecular Genetic Laboratory, Department of Pathology/Lab Medicine, All India Institute of Medical Sciences, Patna-801507, India.
*Corresponding Author:Dr.Ajit Kumar Saxena, Ph.D. Professor and Head Department of Pathology/Lab Medicine, All India Institute of Medical Sciences Patna, Phulwarisharif-801507, Bihar, India, Tel: +91-7781012677; Fax: +91-7781012677; E-mail: draksaxena1@rediffmail.com
Citation: Ajit Kumar Saxena (2023)Circulating Tumor Cells - The Future of Medicine as Diagnostic and Therapeutic Biomarker”. Cancer Prog Diagn 7: 136.
Received: March 22, 2023; Accepted: April 17, 2023; Published: April 20, 2023.
Abstract
Human circulating tumor cells (CTCs) are synonyms of cancer cells, originated from primary tumor sites after activation of oncogenes such as kras and started circulated into the blood stream. These CTCs reach targeted neighbouring tissue or nearby organs, show proliferation and show symptoms of metastasis after invasion. However, identification and characterization of CTCs is challenging task because of very low and heterogeneous population using epithelial mesenchymal transition markers -Sox4, EpCAM and CK 19. Even after technological advancement and use of flowcytometry or RT-qPCR for the study of CTCs required 10-20 ml of blood samples seems to be raise several ethical issues with discordance findings in different types of tumors bearing patient. The author emphasizes the use cell and tissue culture technology and minimal use of sample (0.5ml) from cancer patients, culture for 72 hours under sterile conditions and isolates CTCs by Ficoll’s gradient procedure showing satisfactorily results. The purpose of the CTCs based on cell-culture is to enhance cell population and reduce sample size. The study of CTCs has great clinical relevance as “biological marker” for early diagnosis or before metastasis in breast cancer patients may reduce the incidence of mortality and may help clinicians for better management. However, the biomarkers vary depending upon the cancer. Clinical significance of CTCs is evaluated in breast, lung, ovary, prostate, colorectal, melanoma cancer. Several illustrations had been documented circulating tumor cells may be used as biological marker for monitoring of cancer but still fail for early detection. Hence, a comprehensive review has been written including latest finding of CTCs including clinical significance in diagnostic, prognostic and therapeutic monitoring. Moreover, this review will enhance the knowledge of CTCs and contribute to providing significant knowledge on clinical research for early management.
Keywords
Circulating Tumor Cell, Cancer Biomarker, Breast, Colorectal, Liver Cancer.
Introduction
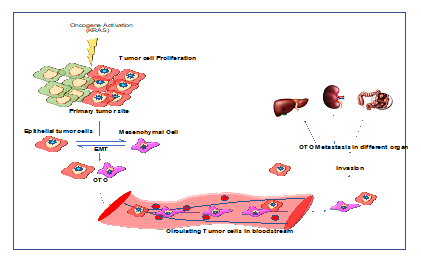
During tumorigenesis, cells undergo epithelial to mesenchymal transition (EMT) and separated from the primary tumor site, travel through the vascular system are called circulating tumor cells (CTCs) (1). The dissemination process of CTCs is still under investigation, however, preliminary studies showed tumor cells migrate via localized invasion of basement membrane during primary tumor progression(2). Further, they intravasate into bloodstream or lymphatic systems (3), during circulation they interact with blood components for survival by competing with immune cells, and shear stress. However, during circulation most of the CTCs died while some of them survive, extravasate, migrate and colonise to form micro metastases followed by angiogenesis and grown into metastatic tumors (4,5). However, during this process only few (> 0.01%) of the CTCs metastasize (6) (Figure 1.).
CTCs intravasate into bloodstream encounter series of hostile environmental changes including immune attacks, shear stress, anoikic, oxidative stress and the lack of cytokines and growth factors (6). During this process only a few of the CTCs survived. CTCs are similar to mesenchymal cells thus, during primary tumorigenesis the EMT process is vital to understand the transition of epithelial cells to mesenchymal cells (7). During the EMT, epithelial cells lose epithelial characteristics such as the expression of EpCAM, keratins, and E-cadherin and upregulate matrix metalloproteinase (MMP) activity, which enables these cells to navigate through the local extracellular matrix (ECM) and enter the microvasculature(8–10). Thus, CTCs can be easily separated from primary tissue, invade the capillaries and possess a significantly improved ability to survive and metastasize. The presence of CTCs in bloods were first reported back in 1869 by Ashworth Thomas Ramsden, revealing the size, shape, and properties similar to the primary tumor (11). Since then, several groups have focused on development of CTCs detection technique and diagnostic potential to assess the tumor heterogeneity (11,12). Several studies reported the presence of CTCs in different cancers including lung, prostate, breast, gall bladder, and ovary (13–15). The CTCs detection, characterization and their potential in diagnostics, prognostics and therapeutics has been evaluated over the past two decades. However, several obstacles are accompanying the isolation, and detection of CTCs. First, CTCs are rarely available in blood stream. Around 1–5 cells are only found in millions of blood cells per 7.5 mL of blood (16,17). Moreover, CTCs cells are heterogenous, therefore, variation in expression of cell surface marker (8,18). Therefore, it is not easy to recognize different types of CTCs by the identical standard (19). Herein, we systematically review CTCs in different cancers, potential as diagnostics, prognostics and therapeutic molecules in different cancers. During this systemic review we used keyword “CTC, CTCs in different cancer, CTCs in diagnosis of cancer, CTCs as prognostic biomarker, CTCs as therapeutic agent” and many more in google search engine, PubMed, Google Scholar to find past and current literature for review. We briefly reviewed CTCs biology, advancement of CTCs in different cancers, and investigated the diagnostic, prognostics and therapeutic potential of CTCs in different cancers. Moreover, the clinical significance of CTCs is extrapolated in terms of significance in monitoring cancer progression. Although the detection of CTCs is a promising technique for precision medicine, notably, there are still many unsolved problems. In this review, we present the existing challenges and offer our own insights into the future development of CTCs.
Circulating Tumor Cells in Cancer
Circulating-Tumor-Cells (CTC) provide a blood biomarker for early carcinogenesis, cancer progression and treatment effectiveness. An increase in CTCs is associated with cancer progression, a CTC decrease with cancer containment or remission (20). The presence of CTC has also been associated with early carcinogenesis and risk of cancer (21). Discovery of CTCs opens new insight in understanding of metastatic cancer and its progression. Several cancers have been reported to disseminate via CTCs including breast, prostate, pancreas, gall bladder, ovary cancer etc. Herein, we briefly describe the recent progress in CTCs based study in different cancers.
Figure 1: Diagrammatic presentation of biogenesis of CTC during course of tumor formation and epithelial mesenchymal transition.
Circulating Tumor Cells in Breast Cancer
In 2020, breast cancer surpassed lung cancer as the most prevalent type of cancer worldwide. The metastatic nature of cancer is of great concern accounting for 90% of cancer-related deaths in breast cancer patients (22). One theory confers that tumor metastasis is triggered by blood-based CTC (23). Cristofanilli et al revealed the prognostic value (PFS and OS) of CTC in metastatic breast cancer patients having cut-off of 5 CTC/7.5 ml of blood using CellSearch system (24). Hence, this study transformed the applicability of CTC in several cancer types. Since, several studies have been conducted on enumeration of CTCs in metastatic breast cancer and correlated with clinical significance (25,26).
A recent study evaluated the clinical efficacy of CTC quantification for the prognostication of patients with metastatic breast cancer in 1944 different patients by the Cell Search method at baseline (before start of new treatment). According to the authors, normalization for CTC levels at baseline in early treatment, the shorter PFS was linked to higher CTC counts between three- and five-weeks providing role in prognosis of breast cancer patients (27). In accordance with the most recent recommendations, hormonal therapeutics and anti-HER-2 treatments are provided for breast cancer patients based on the underlying tumor's hormones (ER/PR expression) and HER-2 status. The hormone receptor and HER-2 status in CTC, particularly during disease recurrence or progression in breast cancer patients, can differ from that in primary tumors and even change over time, according to a growing body of research (28,29). Accordingly, molecular characterization of CTCs hormone receptor and HER-2 status could be used as optional personalized treatment and have potential for clinical use (30,31). In the metastatic cascade, the mechanism of epithelial-mesenchymal transition (EMT) is crucial (32,33). CTC molecular evaluation highlights the significance of EMT, which is essential for enabling malignancies to penetrate and thrive at remote sites from the tumor origin. The evaluation of EMT-inducing TFs expression profiles has been assessed in CTC patients with primary breast carcinoma. (34).
Similarly, CTCs expressing stemness markers have significant effects on treatment resistance. Patients with metastatic and early breast cancer were shown to have a high percentage of CTCs that exhibit EMT and tumor stem cell features as well as CTCs that express TWIST and vimentin (35,36). The existence of a subpopulation of CTCs with putative stem cell progenitor phenotypes in patients with metastatic breast cancer has been shown by using triple-marker immunofluorescence microscopy (37). Currently used detection methods for CTC are not efficient to identify this subtype of CTC which underwent EMT (38). Moreover, studies on the molecular characterization of CTCs have revealed that CTCs even within the same patient are heterogeneous. In non-metastatic breast cancer patients, the expression of estrogen, progesterone and epidermal growth factor receptor (EGFR) by immunofluorescence experiments revealed heterogeneous expression of these hormonal receptors in samples from the same patients.
Recently, Jin, et al. reported CTCs could be used as marker for diagnosis and staging of breast cancer patients with the diagnostic value of 86% with 95.4% specificity and 76.56% of sensitivity (39). Similarly, Zhou et al reported the 81% of preoperative patient’s blood samples were CTCs marker positive, while, after surgery around 67.1% patient’s turnout to have negative status with respect to CTCs marker in blood and could aid in therapeutic and disease progression (40). Recent study by Pang et revealed prognostic value of CTC treated with pre-adjuvant chemotherapy and post adjuvant chemotherapy breast cancer patients undergoing surgery. The count of CTCs was having significant correlation with progression free survival and overall survival of patients (14). Similarly, Krol et al, revealed presence of CTC cluster in early breast cancer are possible risk factors for progression of disease (41). In another recent study, Carlotta et al, revealed CTC positive patients have poor overall survival compared to CTC negative patients. Moreover, NGS sequencing of CTCs showed high genomic instability and mutation (42). Recent, clinical trial-III (NCT01619111) revealed that CTC count could serve as biomarker for metastatic breast cancer. The recent development and clinical significance of CTCs in breast cancer are tabulated in table 1.
Table 1: Clinical Significance of CTCs Detection in Breast Cancer Patients.
|
Methodology |
Year |
Patients |
Clinical relevance |
Ref |
|
CytoSorter® |
2022 |
343 |
Diagnostic Value |
(43) |
|
CellSearch® |
2022 |
3754 |
Therapeutic monitoring |
(44) |
|
Immunomagnetic nanospheres (IMNs) |
2021 |
164 |
PFS, OS |
(45) |
|
CytoSorter® |
2020 |
396 |
Diagnostic Value |
|
|
CellSearch & Ficoll based method |
2019 |
57 |
Decrease in overall survival |
(42) |
|
CellSearch® |
2018 |
547 |
Disease Recurrence |
(46) |
|
CellSearch® |
2018 |
546 |
Disease Recurrence |
|
|
CellSearch® |
2010 |
115 |
DFS, OS |
(48) |
|
RT-PCR |
2009 |
165 |
OS1 |
(49) |
|
CellSearch® |
2008 |
118 |
DFS3 |
(50) |
Circulating Tumor Cells in Prostate Cancer
The FDA has approved CTC enumeration for use in monitoring advanced disease in prostate cancer after it was thoroughly examined and verified as a prognostic tool. We searched published articles Google Scholar, PubMed, and Science Direct with specific keywords (CTCs in prostate cancer, CTCs in prostate cancer therapeutics, CTC as biomarker of prostate cancer), in return more than 150 studies were observed. The FDA has approved CTC enumeration utilizing the Veridex CellSearch TM system for estimation of burden of tumor cell spread in baseline and post therapeutic patients advance stage prostate cancer patients. This test is being used as standard clinical practice to predict the survival, and effectiveness of treatment (51).
In addition, the innovative anti-androgen treatments abiraterone acetate and MDV3100 are currently being investigated in major phase III trials to determine the clinical value of tracking CTC changes with treatment as an efficacy-response surrogate biomarker of survival (52). It is possible to identify and define molecular factors in CTC as predictive biomarkers of tumor sensitivity to a treatment approach (53). Latest studies have gone into greater depth on the major CTC research in metastatic and localised prostate cancer, showing the significant benefits as well as the difficulties presented by diverse techniques, especially potential implications for improving prostate cancer care (30).
In 2001, Moreno, et al. were the first to reveal the blood CTC level of patients with advanced prostate cancer and correlated the CTC levels with disease development with no diurnal variation over time (54).Later, in 2007, Danila and colleagues revealed that CTC count before therapy offers specific information on prognosis as well as the release of cells into the bloodstream is a characteristic of the tumor that is distinct from the severity of the disease (55). In 2008, de Bono and colleagues reported CellSearchTM system based enumeration of CTC in patients with metastatic castration- resistant prostate cancer (CRPC) has prognostic and predictive value and could be used as independent predictor of OS in CRPC, enabling the FDA to approval for the assessment of CRPC (56).CTC counts are able to track the status of the disease and, when examined as a continuous variable, can determine OS and provide independent prognostic information of disease development (57). Resel et al, examined the relationships among CTC count and PSA level, Gleason scores, and TNM stages of patients with malignant hormone-sensitive prostate cancer revealed the CTC from blood could accurately stage the prostate cancer and have prognostic value assessment of metastatic hormone-sensitive prostate cancer (58)
Combining CTC and PSA kinetics may provide knowledge on management and diagnosis of advanced prostate cancer (59,60). Recently, detection of CTCs in early prostate cancer and may be utilized as a novel surrogate marker for systemic and local treatment (61). Another study revealed the presence of CTCs in early stage of prostate cancer could be used as surrogate biomarker, moreover, reduction of CTC number in post treatment could be indicator of therapy response (62). Prostate cancer development is dependent upon the androgen receptor (AR) signaling. The enhanced expression of splice variant of androgen receptor helps in disease progression and is induced by androgen ablation therapy. Intervention of Taxane based CRPC therapy gold standard, a recent finding suggests the relationship of spliced androgen receptors (ARv567 and Arv7) with microtubules and dynein motor protein resulting in differential sensitivity toward taxane in cell line as well as in vivo system (63). In addition, discovery of ligand mediated AR signaling in CRPC enhances the use of abiraterone acetate (AA), an androgen biosynthesis inhibitor, which increases the patient’s survival rate. Miyamoto et al, demonstrated that assessment of AR signaling in blood derived CTC may aid to guide therapy in metastatic prostate cancer (64,65). In recent study by Ried et al, revealed diagnostic value of CTC in detection of prostate cancer by combining prostate specific marker. The blood based ISET® CTC assay showed 99% of positive predictive value and 97% of negative predictive value in diagnosis of prostate cancer (66). In another study, Yang et al reported telomerase-based CTC detection (TBCD) method of prostate cancer. The diagnostic value based on ROC analysis was 78.9% (67). The recent development in field CTCs based clinical application in prostate cancer is depicted in table 2.
Table2: Clinical Significance of CTCs in Diagnosis and Prognosis of Prostate Cancer.
|
Methodology |
Year |
Patients |
Clinical relevance |
|
|
Telomerase-based CTC detection (TBCD) |
2021 |
203 |
Diagnostic Value |
(67)
|
|
ISET® |
2020 |
2000 |
Diagnostic value |
(66) |
|
CellSearch & RT-PCR |
2020 |
243 |
Diagnostic and Disease recurrence |
(75)
|
|
CellSearch® |
2019 |
37 |
Recurrence |
|
|
CellSearch® |
2018 |
511 |
Diagnostic and prognostic value |
(77)
|
|
CellSearch® |
2018 |
44 |
Early Diagnosis |
(78) |
|
CellSearch® |
2018 |
6081 |
Treatment Efficacy |
(79) |
|
Conventional Method |
2017 |
162 |
Prognostic value, OS, PFS |
(80) |
|
CellSearch® |
2016 |
30 |
Monitoring |
|
|
CellSearch® |
2008 |
276 |
Overall Survival |
(56) |
Circulating Tumor Cells in Lung Cancer
According to the World health organization (WHO)-2020 report, around 2.21 million lung cancer cases were reported worldwide. Online data curation on NIH official website, and other online resources (Google Scholar, Science Direct, PubMed, and Research Gate) showed 350 studies based on CTC in Lung cancer when we used keyword “CTC in Lung Cancer, CTC based diagnosis of Lung cancer, Prognostic and therapeutic role of CTC in lung cancer”. In lung cancer, CTCs frequently display non-epithelial features. Moreover, the majority of detection techniques rely on epithelial markers to identify the CTCs and loss of these markers during EMT in some metastatic tumors can make these techniques useless. Hence, CTC detection in lung cancer has proven a challenging task. There are no established biomarkers for predicting therapeutic efficacy in non-small-cell lung cancer (NSCLC). Zhu et al revealed the EpCAM/MUC1 positive CTC patients have significantly lower DFS and OS in pre-surgery and post-surgery patients (68). Recently, existence of hybrid CTCs (epithelial/mesenchymal) in NSCLC patients was discovered using EpCAM independent blood filtration system (isolation by size of epithelial tumor cells (ISET) and immunofluorescence). Moreover, further characterization can provide significant insight on role of CTCs in EMT and metastases process in NSCLC patients (69). Similarly, another study revealed the prognostic value of CTCs and could tell us about the early therapeutic relevance in NSCLC patients (Stage III-IV) (70). Hou, et al. revealed the clinical and molecular significance of CTC and clustered CTC in SCLC patients. The variation in baseline CTC count of prechemotherapy and post chemotherapy could be used as prognostic factor in SCLC patients (71). In another study by Haber et al showed the EGFR mutation in CTCs from lung have progressive disease than the non-mutated EGFR CTCs in lung cancer patients (72). In another study by, et al. revealed diagnostic potential of CTCs in cohort of 302 lung cancer patients (73). Li, et al. reported the diagnostic value of CTC in detection of lung cancer with AUC of 0.975, sensitivity of 87.5% and specificity of 95.7% (74). Recent study evaluated clinical significance of CTC in prostate cancer are listed in table 3.
Table 3: Study involving CTCs for Evaluation of Diagnostic and Prognostic value in Lung Cancer.
|
Authors |
Technique used |
Number of patients |
Clinical relevance |
|
|
Hofman, et al., 2010 |
ISET® |
208 P + 39 N |
Prognostic value |
(82)
|
|
Horfman, et al., 2012 |
ISET® |
250 P + 59 N |
Prognostic Value |
(83) |
|
Devriese, et al. 2012 |
MACS®+qF PCR |
46P + 46 N |
Diagnostics & Prognostic Value |
(84) |
|
Punnoose, et al., 2012 |
CellSerachTM |
37 P |
Prognostic and Therapeutic relevance |
(85) |
|
Ilie, et al., 2014 |
ISET® |
168 COPD P +77 N |
Cancer progression |
(21) |
|
Zhang, et al., 2016 |
Cyttel (negative immune-magnetic selection |
46 P |
Prognostic value |
(86) |
|
Crosbie, et al., 2016 |
CellSerchTM |
30 P |
Prognostic Value |
(87) |
|
Coco, et al., 2017 |
ScreenCell |
73 P |
Prognostic Value |
(88) |
|
Tong, et al., 2017 |
Cyttel |
127 P |
Prognostic and Recurrence |
(86) |
|
Ilie, et al., 2017 |
CellSearchTM & ISET® |
362, (ISET®) |
Diagnostic value |
(21)
|
|
Turetta, et al., 2018 |
Flow Cytometry |
30 P |
Metastases and prognosis |
(90) |
|
Sinoquet, et al., 2021 |
CellSearchTM |
54 P |
Therapeutic relavance |
(91) |
|
Lu, et al., 2021 |
FlowCell System |
306 P |
Diagnostic and predictor of metastasis |
(73) |
|
Li, et al., 2021 |
imFISH |
56 P, 27 N |
Diagnostic biomarker and Therapy monitoring |
(74) |
Circulating Tumor Cells in Colorectal Cancer
Enumeration of CTC by the CellSearch system are promising indicators for the therapy and have a substantial prognostic impact on CRC. The identification of CTCs in localized CRC may assist in determining patients who are at risk for metastasis and categorize patients for adjuvant therapeutic treatment. The counting of CTCs in advanced metastatic CRC can assist risk evaluation, overall therapeutic monitoring, and identification of therapeutic resistance.
A contextual trial has convincingly demonstrated the predictive significance of CTC in patients with colorectal liver metastases or widely disseminated metastatic CRC (92). Several studies reported the importance of CTCs in postoperative blood samples of CRC patients. In preoperative patients the enumeration of CTC acts as an independent prognostic factor indicating recurrence of cancer (93). In a retrospective study, the CellSearch technology was used to evaluate the CTC in 430 metastatic colorectal cancer patients at baseline and after beginning first-, second-, or third-line therapy. This analysis revealed that PFS and OS in patients having mCRC were independently predicted by the CTC count before and during treatment leading to the FDA approval of CellSearch assay for mCRC (94). Furthermore, it was demonstrated that evaluating CTC count before and during course of treatment could reliably reflects PFS and OS in late-stage CRC patients undergone chemotherapy plus targeted drugs, moreover, they add on more insight to CT imaging (95). Further research demonstrated the clinical efficacy of CTC count in enhancing the clinician's capacity to precisely assess the outcomes of oxaliplatin-based therapeutic treatment and in accelerating the identification of efficient treatment regimens for specific patients (96).
Similarly, another study on patients undergoing chemotherapy revealed a significant relationship between both the CTCs count and the advancement of the cancer as seen on radiographs (97). Barbazan, et al. evaluated the therapeutic usefulness of six CTC markers (tissue specific and EMT transcripts) as predictive and prognostic markers in patients with mCRC. Patients who were therapy-refractory but were missed by conventional imaging approaches were found using CTC-markers. Patients identified by computerized tomography as respondents but with elevated CTC markers throughout therapy had considerably shorter life durations (98).
Compared to mCRC, the predictive value of CTC in non-metastatic CRC is less evident. Due to the lower CTC count in non-metastatic CRC, particularly precise and intuitive detection techniques are needed. Recent study, focusing on detection procedures and prognostic value, investigated the potential clinical importance of CTC in non-metastatic CRC (TNM-stage I–III). Based on the observations, patients with non-metastatic colorectal cancer who have CTC in their bloodstream may have a worst DFS (99). Enumeration of CTC using FDA approved CellSearch technology may aid in the identification of high-risk stage II CRC patient candidate for adjuvant treatment (100). Iinuma, et al. assessed the clinical importance of blood-based CTCs of post-surgical CRC patients as a predictive factor for overall survival and disease-free survival using CEA, CK, and CD133 as genetic markers. Patients with positive results for these markers in the training sets had significantly worse overall survival and disease-free survival than patients with negative results (101). In order to determine the effectiveness of anti-EGFR therapy in treating metastatic CRC, initial tumors are examined for the existence of KRAS and BRAF mutations. However, differences in KRAS and BRAF mutation level across primary, CTC, and metastatic tumors in patients with advanced colorectal cancer have significant ramifications (29).
Similarly, Gasch C, et al. used the CellSearch method to evaluate expression of EGFR expression, EGFR gene amplification, and KRAS, BRAF, and PIK3CA mutations in single CTCs from patients with metastatic (102). Similarly, another study on single CTC isolated from CRC patient revealed the KRAS mutational correlation among CTCs and primary tumor in around 50% of matched instances (103). Similarly, evaluation of primary and metastatic samples of matched patient revealed presence of mutation of APC, KRAS and PIK3CA at sub clonal level (104). Compared to the traditional tumor marker CEA, CTCs are more promising markers for the assessment and forecasting of treatment outcomes in patients with rectal cancer. Evaluation of clinical relevance of CTCs in comparison to CEA shows strong association among CTC counts and patient response, while serum CEA doesn’t establish any correlation (105). Recent study signifying clinical significance of CTC in colorectal cancer are tabulated in table 4.
Table 4: Study involving CTCs for evaluation of Diagnostic and Prognostic value in Colorectal Cancer.
|
Authors |
Technique used |
Patients No. |
Clinical relevance |
|
|
Yu, et al. |
Cyttel Method |
89 |
Diagnostic value |
(106) |
|
Dizdar, et al. |
CellCollector |
80 |
Prognostic value |
(107) |
|
Pan, et al. |
Density gradient |
163 |
Prognosis & Staging |
(108) |
|
Baek, et al. |
FAST Technique |
88 |
Diagnosis & prognosis |
(109) |
|
Yang, et al. |
ISET® |
138 |
Prognostic value |
(110) |
|
Wang, et al. |
Meta-Analysis |
NA |
OS, PFS |
(111) |
|
Yu, et al. |
CellRichTM |
76 |
DFS, Therapeutic monitoring |
(112) |
|
Xiong, et al. |
ISET® |
89 |
OS, PFS |
(113) |
|
Hendricks, et al. |
ScreenCell® |
57 |
Diagnostic value |
(114) |
|
Silva, et al. |
ISET® |
54 |
Diagnostic & Therapeutics |
(115) |
|
Tol, et al. |
CellSearch® |
451 |
Overall Survival |
(95) |
|
Cohen, et al. |
ISET® |
430 |
Prognostic value (OS & PFS) |
(116) |
|
Lalmahomed et al |
CellSearch® |
173 |
Overall Survival |
(117) |
Circulating Tumor Cells in Melanoma Cases
Cutaneous melanoma develops when epidermal melanocytes change into melanoma cells, a process that is commonly linked with harmful prolonged ultra-violate exposure (118). CTCs from cutaneous and acral melanomas are almost certain to metastasize to other organs (118,119). Metastasis and migration of melanoma CTCs in different organs of body has unique properties and make them special as compared to other solid tumors (120). In recent years, qRT-PCR based single plex or multiplex biomarkers has emerged as a popular tool for melanoma CTC evaluation. The melanoma genes should be constitutively expressed in melanoma tumors and CTCs, compared to PBMCs healthy patients. To overcome heterogeneity of tumor and CTC, numerous biomarkers have already been evaluated. The expression of MMA specific gene is heterogeneous and major challenge. Diagnostic and treatment of melanoma is highly dependent upon the heterogeneity of tumor and variable expression of MAA biomarker. Therefore, evaluation of multiplex-gene expression in CTCs has been a crucial strategy for increasing test sensitivity, especially in patients with lower CTCs count. Enhanced sensitivity and specificity are key to anticipating the possible spread of metastases and therapeutic response. In addition, comprehensive analysis of transcriptome, mutation-based expression analysis of genes or related pathways become highly evident in Cancer Genome Atlas (TCGA). Additionally, the FDA-approved monoclonal Antibody-based checkpoint inhibitor immunotherapies (CII) and several small molecule inhibitors (SMI) for MMA patients provide increased relevance on CTC measurement in monitoring outcomes (121).
CTC presence in patient’s blood is often related with advance-stage metastatic MMA with poor PFS. qRT-PCR based expression analysis of MART-1, MAGE-A3, and PAX3 gene in CTC shown to have higher expression in stage-IV MMA 54%), and the CTC in blood was substantially linked with DFS and OS (122). Kiyohara et al, evaluated a panel of marker using qRT-PCR technique for direct CTC identification, instead of CTC fractionation from leukocytes. The assay constitutes MART-1/Melan-A, MAGE-A3, PAX3, and GalNAc-T gene and shown to have higher sensitivity, specificity toward detection of CTC with crucial clinical application (123). In addition, uveal melanoma termed as most deadly ophthalmological illnesses. Therefore, it requires biomarkers that can foretell the advent of metastases. In recent study, with lengthy follow-up duration, revealed CTC as negative prognostic biomarker in uveal MMA patients. Moreover, CTCs molecular characterization will certainly add in interpretation of metastasis and could enhance patients care (124). Using CTC profiling, this might be possible to identify MMA patients who could benefit from intensive adjuvant therapy or to group individuals for adjuvant clinical trials. Sentinel lymph node (SLN) metastases in MMA patients may result in a wide variety of conditions, rendering it difficult to reach agreement on their course of care. Identification of high-risk individuals from clinical context may aid with prognostic and treatment planning. Hoshimoto et al, assessed the clinical significance of multiplexed biomarker panel (MART-1, MAGE-A3, and GalNAc-T) using qRT-PCR for identification of CTC from SLN metastasized MMA after complete lymphadenectomy. Result revealed 13.4% to 17.5% of detection range for single CTC biomarker without any disease correlation. However, detection of more than one CTC biomarker was substantially linked to lower recurrence-free survival, distant metastasis, and disease-free survival (122). Assessment CTC level in blood of melanoma patients could be used to evaluate progression and therapy response (125). Moreover, advancement in molecular characterization of CTC may provide new personalized therapeutic approaches for management of disease (126). Recent published study providing clinical significance in melanoma cancer are listed in table 5.
Table 5: Represent study involving CTCs for evaluation of Diagnostic value in Melanoma cancer.
|
Author/Ref. |
Patients no. |
CTC Enrichment/ Detection |
CTC Markers |
Stage |
Findings |
|
I Samija, et al./ 2010 (127) |
201 |
MM PCR |
MITF, TYR |
I-IV |
Survival (OS, PFS) |
|
C Rao et al/(128) |
44 |
CELLSEARCH® |
CD146, HMW-MAA |
III, IV |
Survival (OS) |
|
S Hoshimoto, et al./ (122) |
244 |
MM PCR |
MAGEA3, MLANA, PAX3 |
IV |
Survival (DFS, OS) |
|
AL Reid, et al./(122) |
230 |
MM PCR |
ABCB5, MCAM, MLANA, PAX3, TGFB2, PAX3 |
0–IV |
Recurrence, Treatment response |
|
ES Gray, et al./ (129) |
56 |
Flow cytometry |
ABCB5, CD146, CD271, HMW-MAA, RANK |
I–IV |
Survival (PFS) |
|
J Li, et al./ (130)
|
100 |
CELLSEARCH® |
CD146, HMW-MAA |
I–IV |
AJCC Stage, Survival (OS, PFS, DSS) |
|
CS Hall, et al./ (131) |
93 |
CELLSEARCH® |
CD146, HMW-MAA |
IV |
Survival (PFS) |
|
A Lucci et al/.(132) |
243 |
CELLSEARCH® |
CD146, HMW-MAA |
III |
Survival (RFS) |
|
SY Lin, et al./ (133)
|
75 |
ClearCell® FX/MM PCR |
B4GALNT1, MAGEA3, MLANA, PAX3, TRP-AGG2-6 |
III, IV |
Survival (DFS, OS), Treatment response |
CTC: circulating tumor cell, DFS: disease-free survival, OS: overall survival, DDFS: distant-disease free survival, PFS: progression-free survival, RFS: recurrence-free survival.
Circulating Tumor Cells in Pancreases
According to Cancer Research Statistics-2022, pancreatic carcinoma ranked fourth in terms of morbidity in the USA and Europe. The incident rate and mortality are equal with overall five-year survival rate of <6% (134) and will become second morbidity causing cancer by 2030 (135). The poor recovery of pancreatic carcinoma patients is often associated with hyper-metastasis of tumor at early stage without symptom. The frequent dissemination of pancreatic cancer to other organs revealed their potential of migrating through the circulating system. Therefore, evaluation of CTC count in blood could be used as liquid based diagnostic and prognostic biomarker for pancreatic cancer. In recent decades CTCs clinical significance has been extensively explored in several cancers along with pancreatic cancer, however, complete significance of CTCs has not been explored in pancreatic cancer. However, the presence of CTCs in benign pancreatic neoplasm stimulated researchers to identify the role of CTCs in diagnosis, prognosis and metastasis extensively studied in pancreatic tumor (136,137). Several studies reported the prognostic role of CTCs in different pancreatic cancer (Table 1). Conventionally, tumor size, nodal status, and perineural invasion were associated with prognostic factor and require surgical resection. Hereby, CTCs shows difference as they are minimally invasive and look into the developmental as cancer progression. Martini, et al., suggested the CTC presence in pancreatic cancer patients have clinical relevance and have unfavorable outcome (138). In another study, enumeration of CTC in pancreatic carcinoma patients using CellSearch® system revealed to have positive association with poor tumor differentiation and smaller had a significantly lower PFS, moreover, CTC-positive group had a lower OS than patients in the CTC-negative group (140). Bidard, et al. evaluated CTCs in locally advanced PDAC patients and reported 11% of CTC-positive patients with worse overall survival (141). Similarly, another study reported the MTHFR C677T and CK19 mutation in CTCs isolated from the blood of pancreatic tumor patients (142). However, variation in result is more often due to CTC enumeration technique and patients. To gain a deeper understanding of the clinical consequences of CTC discovery in pancreatic cancer patients, further investigations and characterization of the CTC population are needed. Recent study involving CTC in pancreatic cancer are depicted in table 6.
Table 6: Represent study involving CTCs for evaluation of diagnostic and prognostic value in pancreatic cancer.
|
Author/ Ref. |
Sample no |
Stages |
Technique |
Significance |
|
Soeth, et al., /(143) |
172 |
All stages, |
Ficoll’s based |
CTC+: poor OS |
|
Hoffmann, et al., / (144) |
37 |
All stages |
Ficoll’s based |
CTC+: worse OS |
|
Kurihara, et al., /(145) |
26 |
Stage III and IV |
CellSearch® |
CTC+: worse OS |
|
Khoja, et al., / (146) |
54 |
NA |
ISET®; CellSearch® |
Decreased OS |
|
De Albuquerque, et al.,/(97) |
34 |
All stages (II–IV) |
Immunomagnetic (EPCAM) |
CTC + worse PFS |
|
Bidard, et al., / (147) |
79 |
NA |
CellSearch® |
CTC+ worse OS |
|
Bissolati, et al., / (148) |
20 |
Stage IIa and b |
CellSearch® |
CTC+ metastasis |
|
Zhang, et al., / (149) |
22 |
Stage I–IV, |
Immunomagnetic (CEP 8/ CD45) |
CTC+: worse OS |
|
Earl, et al., / (150) |
35 |
Stage II–IV |
CellSearch® |
CTC+: worse OS, |
|
Poruk, et al., / (151) |
60 |
All stages |
ISET® |
Epithelial CTC+: earlier recurrence |
|
Gao, et al., / (152)
|
25 |
All stages |
CD45 depletion and SE-FISH |
lower CTC count, increase OS |
|
Kulemann, et al., / (153) |
58 |
All stages |
ScreenCell® |
CTC+: worse OS |
|
Okubo, et al., /(141)
|
65 |
III–IV |
CellSearch® |
CTC+ worse OS, Liver metastases, |
|
Poruk, et al., /(154)
|
60 |
Stage I and II |
ISET® |
CTC+TIC (tumor initiating cell): predict decrease in OS and PFS |
|
Gemenetzis, et al., / (155)
|
165 |
All stages |
ISET® |
CTC counts+ recurrence. |
Circulating Tumor Cells in Ovarian Cancer
According to the world cancer research foundation (WCRF-2020), the ovarian cancer (OC) burden annually increases by 6.6%, accounting for 313,959 new cases a year. While morbidity rate was 4.2, accounting for 207,252 deaths. The early diagnosis of OC is still compromised, and the majority of patients are detected at advanced stages. Early diagnosis and prognosis of OC is critical for management of disease, however, the current biomarker regime failed to do so. Liquid biopsy-based biomarker such as cell free DNA, Methylation based biomarker, miRNA, and circulating tumor cells bring new possibility of early diagnosis of OC. Circulating tumor cell-based studies are flourishing in recent decade for evaluation of their potential in diagnosis, prognosis and management of cancers. Several studies reported the clinical relevance of CTC in diagnosis, prognosis and therapeutic monitoring in ovarian cancer (156)
. Lou et al, revealed the predictive value of CTC in ovarian cancer patients, CTC count was significantly elevated in metastatic OC patients than in primary ovarian cancer patients (157). In another study, Yang, et al. reported the clinical significance of CTC count in ovarian cancer, where increase in CTC was associated with higher recurrence rate as compared to patients with lower CTC count (158). Study by Perl, et al. revealed the CTC enrichment based on cell adhesion matrix (CAM) has sensitivity of 83% and specificity of 95% for detecting OC (159). Similarly, Zhang, et al. reported early diagnostic value of CTC, moreover, they revealed the EpCAM-positive CTC could help in prognosis and treatment monitoring (15). Obermayr, et al. reported RT-PCR based detection of six genes isolated from CTC could detect 19 % of the ovarian cancer patients.
In recent study by Zhang, et al. reported the EpCAM positive CTC has diagnostic, and prognostic value along with therapeutic progression monitoring (15). Po et al reported that detection of EpCAM and N-cadherin embedded CTC can enhance the management of ovarian cancer patients (160). Guo, et al. evaluated the diagnostic potential of HE4+ CTC cell in ovarian cancer patients, the AUC, sensitivity, and specificity of HE4+ CTC assay was 71%, 76.7%, and 63% respectively (161). In another recent study, folic acid receptor-based capture of CTC showed 80% sensitivity in ovarian cancer (162). Similarly, Obermayr et al reported the multi-protein marker-based detection of CTC in debulked OC patients for therapeutic stratification (163). Rao, et al. reported microfluidic method conjugated with EpCAM antibody for enumeration of CTC have higher sensitivity in detection EOC patients compared to healthy patients (164). Similarly, lee, et al. evaluated EpCAM+, DAPI+ and CD45 negative feature-based CTC enrichment in EOC patients, result showed to have higher diagnostic and prognostic value (165). Several recent studies have evaluated the diagnostic, prognostic and clinical significance in diagnosis of OC patients based on CTC count. However, conclusive study is still lacking behind their use as biomarkers. Some of the recent research progression in CTC based detection of EOC and their clinical significance are tabulated in table 7.
Table 7: Diagnostic and prognostic value of CTC in diagnosis of ovarian cancer patients.
|
Histotype/Stage |
Sample No: |
Technique used |
Biomarker |
Diagnostic /Prognostic Value |
Ref |
|
|
EOC/I-IV |
109 |
Multiplex RT-PCR |
EpCAM, HER2, MUC1, WT1, P16 and PAX8 |
NR |
OS |
(15) |
|
Primary and recurrent/II, III and IV |
20 |
RT-qPCR |
29 gene markers including: EpCAM, PPIC, MAL2, LAMB1, SERPINE2, TUSC3 |
NR |
NR |
|
|
EOCs (II-IV) |
At diagnosis (102); After treatment (78) |
ICC and FISH |
ICC: EpCAM, Cytokeratins, EGFR, MUC1 and HER2 FISH: MECOM and HHLA1 |
NR |
OS PFS |
|
|
EOC/I-IV |
23 |
ICC |
EpCAM, CK3–6H5, panCK |
NR |
NR |
(164) |
|
EOC/I-IV |
54 |
ICC |
EpCAM, TROP-2, EGFR, Vimentin, N-cadherin |
NR |
HR |
|
|
Serous (24) and non-serous (63)/I-IV |
87 |
ICC |
EpCAM, CK9 |
Sn=77.4%; Sp=55.8% AUC=0.655 |
NR |
|
|
NR |
10 |
ICC |
HE4 and FITC AffiniPure |
Sp=63.3% |
NR |
|
|
EOC |
10 (3 for single- cell analysis) |
Multiplex RT-PCR (AdnaTest) |
19 gene transcripts, including epithelial, EMT and stem cell markers |
NR |
NR |
|
|
EOC/1I-IV |
95 |
Multiplex RT-PCR (AdnaTest) |
EpCAM, ERCC1, MUC1, MUC16, PI3Kα, Akt-2, Twist |
Sn and Sp>90% |
PFS OS |
|
|
EOC/I-IV |
31 |
ICC/RT-qPCR |
ICC: EpCAM, CA-125, CD44, seprase Gene expression: EpCAM, CD44, MUC16 and FAP |
Sn=83%; Sp=97% |
Risk for PD |
|
|
EOC/III and IV |
21 |
FISH, ICC |
CK, CEP8 |
Sn=76.2% Sp> 80% AUC=0.963 (p=0.000) |
NR |
|
|
EOC/I-IV |
129 |
ICC |
EpCAM, ESA, CA-125, DPP4 |
Sn=83% Sp=95.1% |
HR?=?1.06 |
|
|
EOC/I-IV |
143 |
RT-PCR (AdnaTest) |
EpCAM, MUC1, MUC16, ERCC1 |
NR |
OS PFS |
|
|
Serous (173) and non-serous (27)/II-IV |
216 |
RT-qPCR |
12 gene markers including: PPIC, EpCAM, LAMB1, GPX8, TUSC3, TFF1. Also, HE4 |
Sn=22% Sp=85% |
HR? |
|
|
EOC/I-IV |
122 |
RT-PCR (AdnaTest) |
HER-2, MUC1, MUC16, EpCAM |
NR |
HR? |
|
|
EOC |
54 |
ICC |
EpCAM, M30, CK8, 18,19 |
NR |
NS |
|
|
NR |
216 |
ICC |
EpCAM, CK8, 18,19 |
NR |
PFS |
|
Circulating Tumor Cells in Hepatocellular Carcinoma
According to cancer statistics-2018 hepatocellular carcinoma (HCC) ranked as second in terms of morbidity causing cancer and 7th as common cancer (180). Surgical removal, local ablation or transplantation of liver are the most effective way to treat hepatocellular carcinoma, depending upon early diagnosis. However, the current therapeutic approaches have downflow due to higher rate of recurrence (181). The current diagnostic approaches depend upon changes in serum protein marker, histopathological analysis and imaging techniques, however, the sensitivity and specificity is under the question mark. Recent technological advancement in field of liquid biopsy, provided plethora of biomarker (cfDNA, miRNA, circulating tumor cells) having potential in diagnosis of hepatocellular carcinoma at early stage with higher sensitivity and specificity compared to conventional biomarker (182).
Several recent reports evaluated the potential of circulating tumor cells in diagnosis, prognosis and therapeutic monitoring of hepatocellular carcinoma. A recent meta-analysis by Cui, et al. on 1191 patients showed the specificity and sensitivity toward diagnosis of HCC. Moreover, presence higher CTC count in blood increases the risk of hepatocellular recurrence with higher Hazard Ration (183). Winograd, et al. revealed the therapeutic relevance and diagnostic accuracy of CTC in hepatocellular carcinoma (184). Similarly, Saxena, et al. revealed the presence of MTHFR-C677T gene polymorphism and KRAS mutation in CTC isolated from Hepatocellular carcinoma patients increases the risk factor of disease (185).
Clinical Significance of CTCs in Diagnostic, Prognostic, and Therapeutic value
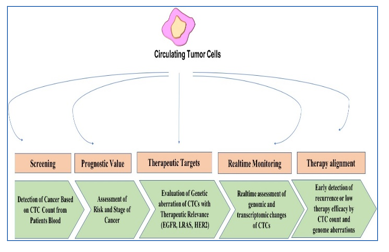
The clinical implication of CTC has been assessed in several solid carcinomas. CTC based enumeration in breast, colorectal and prostate cancer has been approved by FDA for clinical diagnosis. CTC based studies proved to have role in diagnosis, prognosis, screening, therapeutic monitoring, and therapeutic alignment in several cancers (Figure 2). Cristofanilli et al remarked CTC as prognostic biomarker that predicts the PFS and OS of breast cancer patients. This study got FDA approval for clinical application of CTC in breast cancer and further revolutionized the clinical implication of CTC in many cancers (24,186).
Since a CTC test is less costly and non-invasive than a traditional biopsy, it can be repeated frequently throughout treatment. These factors combine to make CTC analysis a potent tool for tracking the progression of cancer. Early diagnosis of breast cancer has great impact on increasing survival of patients, Early diagnosis plays a key role in decreasing mortality of breast cancer, although the grades and breast cancer types have their own importance. For instance, grade I breast cancer progresses considerably more slowly than grades II and III, therefore early detection when tumor diameter is less than two centimeters can improve prognosis and OR (overall survival) of breast cancer patients (187). A recent study evaluated the diagnostic value of CTC in predicting breast cancer with 86.0% of AUC, 95.4% specificity and 76.56% sensitivity (39). Similarly, Yun, et al. revealed the diagnostic potential of CTC in predicting lung cancer with AUC of 93% with 75.0% sensitivity and 89.0% specificity (188). The diagnostic value of CTC at cut-off value of 2 in metastatic colorectal cancer was 90.4% AUC, 83.05% sensitivity and 100% specificity (106). Recently, clinical study by Yang, et al., revealed early diagnostic potential CTC using CellMax biomimetic platform in early colorectal cancer. A total of 620 samples were enrolled with different stages and clinicopathological features. The CTC showed higher early diagnostics accuracy (88%) than routine clinical diagnostics method (189). Similarly, Yasmine, et al. performed LSC-MS analysis (Living single-cell mass spectrometry) and revealed the CTCs complex heterogeneity in single cancer (190). Li, et al. revealed diagnostic potential of CTCs derived genes (CEA, C-Met, MUC1, CK19, EGFR and EpCAM) from 50 CRC patients with 87% sensitivity and 85% accuracy (191). Since now, colonoscopy and biopsy are diagnostic benchmarks, and addition of CTC-positive biopsy could improve the specificity.
Figure 2: Significance of Circulating Tumor Cells in Cancer.
The evaluation of disease progression has been crucial for cancer treatment and prognosis. There have been efforts to incorporate CTC evaluation with well-established diagnostic methods for lung and breast. colorectal, prostate and other cancers. He, et al. concentrated on enhancing the reduced CT screening program's specificity by incorporating CTC examination. CTC numbers were assessed in patients and healthy individuals with detected lung "ground-glass" nodules. CTCs were only found in bloodstream of a small percentage of patients having nodules. Following molecular research, it was shown that these CTCs had a "cancerous predisposition" (192). In another study by Ilie et al evaluated CTC numbers in patients with chronic obstructive pulmonary disease (COPD). Out of 168 patients, only 5 (3%) of them were CTC positive and more interestingly these all five patients got lung cancer in under four years. In addition, no malignancy was discovered in any of the CTC-negative patients during the observational period. These results have been supported by some investigations (193,194). Apart from diagnostics, CTC load could be used in prognosis to predict the recurrence and metastasis. François, et al. revealed the prognostic role of CTC load (higher count) in liver metastatic patients compared to post treatment patients CTC count (195). The CTC count (pre- and post-surgery) plays a vital role in assessment of recurrence and metastasis (196). Similarly, another study revealed the recurrence CRC in postoperative CTC-positive patients (110,197). The ratio of mesenchymal phenotype CTCs to total CTCs can be used to evaluate prognosis and metastasis (198). In addition, the recurrence of breast cancer is a major problem in that increases the burden of cancer and leads to lower survival rate. It is widely acknowledged that early-stage breast cancer malignant tumors have a potent capacity for invasion into distant organs including the bones and lungs.
Basic yet reliable indications of cancer development include CTC count and count fluctuations throughout therapy in many cancer types, thus, CTC count has been shown to be a prognostic predictor (86,199,200). Moreover, evaluation of CTC counts while receiving treatment is a tool that enables evaluation of cancer progression in real time, even before blatant clinical manifestation of relapse. Following surgery and/or chemotherapy, a declining CTC number is most likely an indication of remission. Conversely, a rise in CTC counts signals the recurrence of the disease and should cause the therapy to be revalidated (193,201). According to a recent study, the load of CTCs in blood of pre-therapeutic breast cancer patients has a significant impact on both OR (overall survival) and progression-free survival (24). Rack, et al. study on continuous existence of the CTCs in in pre and post chemotherapeutic patients revealed that the continuous existence of the CTCs in in pre and post chemotherapeutic patients were related with poor overall survival and at risk of recurrence (202). Similarly, Madic, et al. revealed the higher CTC counts in TNBC patients have worst prognosis and lower survival rate (203).
Moreover, post-therapeutic observation of patients is needed for the assessment of disease progression. The CTC count based monitoring of therapy for evaluation of condition has been evidently reported in several studies. During chemotherapy, the clinical utility of CTCs count was evaluated in real-time in breast cancer patients’ data (204). Moreover, a phase-III trials (S0421) validated the prognostic role of CTC count with docetaxel plus prednisone with or without atrasentan for overall survival and diseases response. The baseline CTCs number is prognostic while increasing CTCs at early three weeks signifies worst overall survival, revealing the potential utilization of CTC in therapeutic response measurement (205). Similarly, Sinoquet et al, revealed the PD-L1(+) CTCs from NSCLC patients have poor survival and could be used to predict the anti-PD-1/PD-L1 therapeutic response and resistance (91). In another study Lu et al revealed that CTC could be used as diagnostic marker and predictor metastasis in lung cancer (73). Li et al reported the therapeutic relevance of CTC in lung cancer, post chemotherapy significant decrease in CTC count was associated with enhanced PFS and OS (74).
Conclusion
In the last decade, the increase in cancer burden and morbidity has become a major challenge to the scientists. The early diagnosis of cancer has an impeccable effect on the survival of the patients. Several biomarker regimes have been advocated and approved by FDA for diagnosis of cancer, however the early diagnosis of majority of cancers is still a major concern for clinical scientists. Several cancers are being diagnosed at late stage of disease leading increased morbidity. Circulating tumor cells have been studied enormously in the last two decades for exploitation of their role in metastasis, early diagnosis, prognosis, real-time disease/therapy monitoring. The CTC enumeration method has revealed distinct patterns of expression in different cancers, specifically stages, pre- and post-therapy. The CTC account based approached significantly diagnose the disease at early stage, moreover, they have potential to be used as prognostic marker and could assess the therapy monitoring in real-time. These properties make CTC as a possible biomarker assessment of cancer and disease progression. However, rigorous exploration of CTCs is warranted to validate the clinical application as well as to stand with clinical decision-making compared with other available biomarkers that have been proven and broadly accepted. Nevertheless, CTCs harbor the potential for earlier tumor detection and future, large-scale trials are needed.
Abbreviations:
CTC: Circulating Tumor Cell
EMT: Epithelial Mesenchymal Transition
OC: Ovarian Cancer
HCC: Hepatocellular Carcinoma
PFS: Progression Free Survival
OS: Overall Survival
DFS: Disease Free Survival
HR: Hazard Ration
TIC: Tumor Initiating Cell
TCGA: The Cancer Genome Atlas
AUC: Area Under Curve
EOC: Epithelial Ovarian Cancer
CRC: Colorectal Cancer
PSA: Prostate-Specific Antigen
CRPC: Castration Resistant Prostate Cancer
PBMC: Peripheral Blood Mononuclear Cells
FDA: Food Drug Administration
EGFR: Epidermal Growth Factor Receptor
mCRC: Metastatic Colorectal Cancer
Acknowledgement
We Acknowledge to the Honorable Director, AIIMS Patna, and Department of Science and Technology (Government of India), New Delhi, for providing financial assistance.
Ethics approval and consent to participate:
Ethical approval and consent are not required in the present study.
References
- Dasgupta P, Kulkarni P, Majid S, Hashimoto Y, Shiina M, Shahryari V, et al. (2020) LncRNA CDKN2B-AS1/miR-141/cyclin D network regulates tumor progression and metastasis of renal cell carcinoma. Cell Death Dis 11: 660.
- Weissenstein U, Schumann A, Reif M, Link S, Toffol-Schmidt UD, et al. (2012) Detection of circulating tumor cells in blood of metastatic breast cancer patients using a combination of cytokeratin and EpCAM antibodies. BMC Cancer 12: 206.
- Zavyalova MV, Denisov EV, Tashireva LA, Savelieva OE, Kaigorodova EV, et al. (2019) Intravasation as a Key Step in Cancer Metastasis. Biochemistry Moscow 84: 762–772.
- Szczerba BM, Castro-Giner F, Vetter M, Krol I, Gkountela S, et al. (2019) Neutrophils escort circulating tumour cells to enable cell cycle progression. Nature 566: 553–557.
- Dasgupta A, Lim AR, Ghajar CM (2017) Circulating and disseminated tumor cells: harbingers or initiators of metastasis? Mol Oncol 11: 40–61.
- Micalizzi DS, Maheswaran S, Haber DA (2017) A conduit to metastasis: circulating tumor cell biology. Genes Dev 31: 1827–1840.
- Yeung KT, Yang J (2017) Epithelial-mesenchymal transition in tumor metastasis. Mol Oncol 11:28–39.
- Gires O, Stoecklein NH (2014) Dynamic EpCAM expression on circulating and disseminating tumor cells: causes and consequences. Cell Mol Life Sci 71: 4393–4402.
- Gosens MJEM, van Kempen LCL, van de Velde CJH, van Krieken JHJM, Nagtegaal ID, et al. (2007) Loss of membranous Ep-CAM in budding colorectal carcinoma cells. Mod Pathol 20: 221–232.
- Rejniak KA (2012) Investigating dynamical deformations of tumor cells in circulation: predictions from a theoretical model. Front Oncol [Internet]. [cited 2022 Nov 7] 2.
- Allard WJ, Matera J, Miller MC, Repollet M, Connelly MC, Rao C, et al. (2004) Tumor Cells Circulate in the Peripheral Blood of All Major Carcinomas but not in Healthy Subjects or Patients with Nonmalignant Diseases. Clinical Cancer Research 10: 6897–6904.
- Andree KC, van Dalum G, Terstappen LWMM (2016) Challenges in circulating tumor cell detection by the CellSearch system. Molecular Oncology 10: 395–407.
- Pantel K, Hille C, Scher HI (2019) Circulating Tumor Cells in Prostate Cancer: From Discovery to Clinical Utility. Clinical Chemistry 65: 87–99.
- Pang S, Li H, Xu S, Feng L, Ma X, Chu Y, et al. (2021) Circulating tumour cells at baseline and late phase of treatment provide prognostic value in breast cancer. Sci Rep 11: 13441.
- Zhang X, Li H, Yu X, Li S, Lei Z, Li C, et al. (2018) Analysis of Circulating Tumor Cells in Ovarian Cancer and Their Clinical Value as a Biomarker. Cell Physiol Biochem 48: 1983–1994.
- Miller MC, Doyle GV, Terstappen LWMM (2010) Significance of Circulating Tumor Cells Detected by the CellSearch System in Patients with Metastatic Breast Colorectal and Prostate Cancer. Journal of Oncology 1–8.
- Kulasinghe A, Kenny L, Perry C, Thiery J-P, Jovanovic L, Vela I, et al. (2016) Impact of label-free technologies in head and neck cancer circulating tumour cells. Oncotarget 7: 71223–71234.
- Brasó-Maristany F, Griguolo G, Pascual T, Paré L, Nuciforo P, Llombart-Cussac A, et al. (2020) Phenotypic changes of HER2-positive breast cancer during and after dual HER2 blockade. Nat Commun 11: 385.
- Sharma S, Zhuang R, Long M, Pavlovic M, Kang Y, Ilyas A, et al. (2018) Circulating tumor cell isolation, culture, and downstream molecular analysis. Biotechnology Advances 36: 1063–1078.
- Hayes DF, Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Miller MC, et al. (2006) Circulating Tumor Cells at Each Follow-up Time Point during Therapy of Metastatic Breast Cancer Patients Predict Progression-Free and Overall Survival. Clinical Cancer Research 12: 4218–4224.
- Ilie M, Hofman V, Long-Mira E, Selva E, Vignaud J-M, et al. (2014) “Sentinel” Circulating Tumor Cells Allow Early Diagnosis of Lung Cancer in Patients with Chronic Obstructive Pulmonary Disease. Kalinichenko VV, editor. PLoS ONE 9: e111597.
- Lambert AW, Pattabiraman DR, Weinberg RA (2017) Emerging Biological Principles of Metastasis. Cell 168: 670–691.
- Baccelli I, Schneeweiss A, Riethdorf S, Stenzinger A, Schillert A, Vogel V, et al. (2013) Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat Biotechnol 31: 539–544.
- Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, et al. (2004) Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N Engl J Med 351: 781–791.
- Pierga J-Y, Hajage D, Bachelot T, Delaloge S, Brain E, Campone M, et al. (2012) High independent prognostic and predictive value of circulating tumor cells compared with serum tumor markers in a large prospective trial in first-line chemotherapy for metastatic breast cancer patients. Ann Oncol 23: 618–624.
- Wallwiener M, Hartkopf AD, Baccelli I, Riethdorf S, Schott S, Pantel K, et al. (2013) The prognostic impact of circulating tumor cells in subtypes of metastatic breast cancer. Breast Cancer Res Treat 137: 503–510.
- Bidard F-C, Weigelt B, Reis-Filho JS (2013) Going with the Flow: From Circulating Tumor Cells to DNA. Sci Transl Med 5.
- Riethdorf S, Fritsche H, Müller V, Rau T, Schindlbeck C, Rack B, et al. (2007) Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: a validation study of the CellSearch system. Clin Cancer Res 13:920–928.
- Sieuwerts AM, Mostert B, Bolt-de Vries J, Peeters D, de Jongh FE, et al. (2011) mRNA and microRNA Expression Profiles in Circulating Tumor Cells and Primary Tumors of Metastatic Breast Cancer Patients. Clinical Cancer Research 17: 3600–3618.
- Albin RL, Gilman S (1990) Autoradiographic localization of inhibitory and excitatory amino acid neurotransmitter receptors in human normal and olivopontocerebellar atrophy cerebellar cortex. Brain Res 522: 37–45.
- Turner N, Pestrin M, Galardi F, De Luca F, Malorni L, et al. (2014) Can biomarker assessment on circulating tumor cells help direct therapy in metastatic breast cancer? Cancers (Basel) 6: 684–707.
- Bednarz-Knoll N, Alix-Panabières C, Pantel K (2012) Plasticity of disseminating cancer cells in patients with epithelial malignancies. Cancer Metastasis Rev 31: 673–687.
- Lim J, Thiery JP (2012) Epithelial-mesenchymal transitions: insights from development. Development 139: 3471–3486.
- Mego M, Mani SA, Lee B-N, Li C, Evans KW, et al. (2012) Expression of epithelial-mesenchymal transition-inducing transcription factors in primary breast cancer: The effect of neoadjuvant therapy. Int J Cancer 130: 808–816.
- Kallergi G, Konstantinidis G, Markomanolaki H, Papadaki MA, Mavroudis D, Stournaras C, et al. (2013) Apoptotic circulating tumor cells in early and metastatic breast cancer patients. Mol Cancer Ther 12: 1886–1895.
- Aktas B, Tewes M, Fehm T, Hauch S, Kimmig R, et al. (2009) Stem cell and epithelial-mesenchymal transition markers are frequently overexpressed in circulating tumor cells of metastatic breast cancer patients. Breast Cancer Res 11: R46.
- Theodoropoulos PA, Polioudaki H, Agelaki S, Kallergi G, Saridaki Z, et al. (2010) Circulating tumor cells with a putative stem cell phenotype in peripheral blood of patients with breast cancer. Cancer Lett 288: 99–106.
- Kasimir-Bauer S, Hoffmann O, Wallwiener D, Kimmig R, Fehm T, et al. (2012) Expression of stem cell and epithelial-mesenchymal transition markers in primary breast cancer patients with circulating tumor cells. Breast Cancer Res 14: R15.
- Jin L, Zhao W, Zhang J, Chen W, Xie T, et al. (2020) Evaluation of the diagnostic value of circulating tumor cells with CytoSorter® CTC capture system in patients with breast cancer. Cancer Med 9: 1638–1647.
- Zhou Y (2019) Clinical value of CTC in predicting the efficacy of treatment in breast cancer. JCO 37: e12104–e12104.
- Krol I, Schwab FD, Carbone R, Ritter M, Picocci S, et al. (2021) Detection of clustered circulating tumour cells in early breast cancer. Br J Cancer 125: 23–27.
- Riebensahm C, Joosse SA, Mohme M, Hanssen A, Matschke J, et al. (2019) Clonality of circulating tumor cells in breast cancer brain metastasis patients. Breast Cancer Res 21: 101.
- Shao X, Jin X, Chen Z, Zhang Z, Chen W, Jiang J, et al. (2022) A comprehensive comparison of circulating tumor cells and breast imaging modalities as screening tools for breast cancer in Chinese women. Front Oncol 12: 890248.
- Trapp EK, Fasching PA, Fehm T, Schneeweiss A, Mueller V, et al. (2022) Does the Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer Patients Predict the Site of First Metastasis—Results from the Adjuvant SUCCESS A Trial. Cancers 14: 39-49.
- Pang S, Li H, Xu S, Feng L, Ma X, Chu Y, et al. (2021) Circulating tumour cells at baseline and late phase of treatment provide prognostic value in breast cancer. Sci Rep 11:13441.
- Sparano J, O’Neill A, Alpaugh K, Wolff AC, Northfelt DW, Dang CT, et al. (2018) Association of Circulating Tumor Cells with Late Recurrence of Estrogen Receptor-Positive Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol 4: 1700–1706.
- Sparano J, O’Neill A, Alpaugh K, Wolff A, Northfelt D, Dang C, et al. (2018) Abstract GS6-03: Circulating tumor cells (CTCs) five years after diagnosis are prognostic for late recurrence in operable stage II-III breast cancer. Cancer Research 78: GS6-03-GS6-03.
- Bidard F-C, Mathiot C, Delaloge S, Brain E, Giachetti S, de Cremoux P, et al. (2010) Single circulating tumor cell detection and overall survival in nonmetastatic breast cancer. Ann Oncol 21:729–733.
- Daskalaki A, Agelaki S, Perraki M, Apostolaki S, Xenidis N, Stathopoulos E, et al. (2009) Detection of cytokeratin-19 mRNA-positive cells in the peripheral blood and bone marrow of patients with operable breast cancer. Br J Cancer 101:589–597.
- Pierga J-Y, Bidard F-C, Mathiot C, Brain E, Delaloge S, Giachetti S, et al. (2008) Circulating tumor cell detection predicts early metastatic relapse after neoadjuvant chemotherapy in large operable and locally advanced breast cancer in a phase II randomized trial. Clin Cancer Res 14: 7004–7010.
- Schilling D, Todenhöfer T, Hennenlotter J, Schwentner C, Fehm T, et al. (2012) Isolated, disseminated and circulating tumour cells in prostate cancer. Nat Rev Urol 9: 448-463.
- Han J, Zhang J, Zhang W, Zhang D, Li Y, et al. (2019) Abiraterone and MDV3100 inhibits the proliferation and promotes the apoptosis of prostate cancer cells through mitophagy. Cancer Cell Int 19: 332.
- Danila DC, Anand A, Sung CC, Heller G, Leversha MA, Cao L, et al. (2011) TMPRSS2-ERG status in circulating tumor cells as a predictive biomarker of sensitivity in castration-resistant prostate cancer patients treated with abiraterone acetate. Eur Urol 60: 897–904.
- Moreno JG, O’Hara SM, Gross S, Doyle G, Fritsche H, et al. (2001) Changes in circulating carcinoma cells in patients with metastatic prostate cancer correlate with disease status. Urology 58:386–92.
- Danila DC, Heller G, Gignac GA, Gonzalez-Espinoza R, Anand A, Tanaka E, et al. (2007) Circulating tumor cell number and prognosis in progressive castration-resistant prostate cancer. Clin Cancer Res 13: 7053–7058.
- de Bono JS, Scher HI, Montgomery RB, Parker C, Miller MC, Tissing H, et al. (2008) Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res 14: 6302–6309.
- Olmos D, Arkenau H-T, Ang JE, Ledaki I, Attard G, et al. (2009) Circulating tumour cell (CTC) counts as intermediate end points in castration-resistant prostate cancer (CRPC): a single-centre experience. Ann Oncol 20: 27–33.
- Cie?likowski WA, Antczak A, Nowicki M, Zabel M, Budna-Tukan J (2021) Clinical Relevance of Circulating Tumor Cells in Prostate Cancer Management. Biomedicines 9:1179.
- Helo P, Cronin AM, Danila DC, Wenske S, Gonzalez-Espinoza R, Anand A, et al. (2009) Circulating prostate tumor cells detected by reverse transcription-PCR in men with localized or castration-refractory prostate cancer: concordance with Cell Search assay and association with bone metastases and with survival. Clin Chem 55: 765-773.
- Saad F, Pantel K (2012) The current role of circulating tumor cells in the diagnosis and management of bone metastases in advanced prostate cancer. Future Oncol 8: 321–331.
- Doyen J, Alix-Panabières C, Hofman P, Parks SK, Chamorey E, Naman H, et al. (2012) Circulating tumor cells in prostate cancer: a potential surrogate marker of survival. Crit Rev Oncol Hematol 81: 241–256.
- Lowes LE, Lock M, Rodrigues G, D’Souza D, Bauman G, et al. (2012) Circulating tumour cells in prostate cancer patients receiving salvage radiotherapy. Clin Transl Oncol 14:150-156.
- Thadani-Mulero M, Portella L, Sun S, Sung M, Matov A, et al. (2014) Androgen receptor splice variants determine taxane sensitivity in prostate cancer. Cancer Res 74: 2270–2282.
- Miyamoto DT, Lee RJ, Stott SL, Ting DT, Wittner BS, Ulman M, et al. (2012) Androgen receptor signaling in circulating tumor cells as a marker of hormonally responsive prostate cancer. Cancer Discov 2: 995–1003.
- Steinestel J, Luedeke M, Arndt A, Schnoeller TJ, Lennerz JK, Wurm C, et al. (2019) Detecting predictive androgen receptor modifications in circulating prostate cancer cells. Oncotarget 10: 4213–4223.
- Ried K, Tamanna T, Matthews S, Eng P, Sali A (2020) New Screening Test Improves Detection of Prostate Cancer Using Circulating Tumor Cells and Prostate-Specific Markers. Front Oncol 10: 582.
- Yang Z, Bai H, Hu L, Kong D, Li G, Zhao C, et al. (2022) Improving the diagnosis of prostate cancer by telomerase-positive circulating tumor cells: A prospective pilot study. eClinicalMedicine 43:101-161.
- Zhu W-F, Li J, Yu L-C, Wu Y, Tang X-P, Hu Y-M, et al. (2014) Prognostic value of EpCAM/MUC1 mRNA-positive cells in non-small cell lung cancer patients. Tumour Biol 35: 1211-1219.
- Lecharpentier A, Vielh P, Perez-Moreno P, Planchard D, Soria JC, et al. (2011) Detection of circulating tumour cells with a hybrid (epithelial/mesenchymal) phenotype in patients with metastatic non-small cell lung cancer. Br J Cancer 105: 1338-1341.
- Krebs MG, Metcalf RL, Carter L, Brady G, Blackhall FH, Dive C, et al. (2014) Molecular analysis of circulating tumour cells—biology and biomarkers. Nat Rev Clin Oncol. 11: 129-144.
- Hou J-M, Krebs MG, Lancashire L, Sloane R, Backen A, Swain RK, et al. (2012) Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung cancer. J Clin Oncol 30: 525-532.
- Li S-H, Wu M-H, Wang H-M, Hsu P-C, Fang Y-F, Wang C-L, et al. (2022) Circulating EGFR Mutations in Patients with Lung Adenocarcinoma by Circulating Tumor Cell Isolation Systems: A Concordance Study. IJMS 23:106-161.
- Lu Y, Zheng Y, Wang Y, Gu D, Zhang J, Liu F, et al. (2021) FlowCell-enriched circulating tumor cells as a predictor of lung cancer metastasis. Human Cell 34: 945-951.
- Li Q, Xu C, Yang Z (2021) Circulating Tumor Cells as a Biomarker for Precise Management of Lung Cancer [Internet]. In Review 2021 Jun.
- Xu L, Mao X, Grey A, Scandura G, Guo T, Burke E, et al. (2020) Noninvasive Detection of Clinically Significant Prostate Cancer Using Circulating Tumor Cells. J Urol 203:73-82.
- Friedlander TW, Welty C, Anantharaman A, Schonhoft JD, Jendrisak A, Lee J, et al. (2019) Identification and Characterization of Circulating Tumor Cells in Men Who have Undergone Prostatectomy for Clinically Localized, High Risk Prostate Cancer. Journal of Urology 202: 732-741.
- Lorente D, Olmos D, Mateo J, Dolling D, Bianchini D, Seed G, et al. (2018) Circulating tumour cell increase as a biomarker of disease progression in metastatic castration-resistant prostate cancer patients with low baseline CTC counts. Annals of Oncology 29: 1554–1560.
- Nimgaonkar A, Segurado O, Tsai W-S, Pang S-T, Hou M-F, et al. (2018) A novel circulating tumor cell blood test for early detection of colorectal, prostate, and breast cancers: Results from 709 samples. JCO 36: e13549–e13549.
- Heller G, McCormack R, Kheoh T, Molina A, Smith MR, Dreicer R, et al. (2018) Circulating Tumor Cell Number as a Response Measure of Prolonged Survival for Metastatic Castration-Resistant Prostate Cancer: A Comparison with Prostate-Specific Antigen Across Five Randomized Phase III Clinical Trials. JCO 36: 572-580.
- Qiao Y, Li J, Shi C, Wang W, Qu X, Xiong M, et al. (2017) Prognostic value of circulating tumor cells in the peripheral blood of patients with esophageal squamous cell carcinoma. OTT 10: 1363-1373.
- Kuske A, Gorges TM, Tennstedt P, Tiebel A-K, Pompe R, Preißer F, et al. (2016) Improved detection of circulating tumor cells in non-metastatic high-risk prostate cancer patients. Sci Rep 6:39736.
- Hofman V, Bonnetaud C, Ilie MI, Vielh P, Vignaud JM, Fléjou JF, et al. (2011) Preoperative circulating tumor cell detection using the isolation by size of epithelial tumor cell method for patients with lung cancer is a new prognostic biomarker. Clin Cancer Res 17: 827–835.
- Zeller J (1990) [Neuro-imaging and neurofibromatosis]. Ann Dermatol Venereol 117: 433-435.
- Devriese LA, Bosma AJ, van de Heuvel MM, Heemsbergen W, Voest EE, Schellens JHM, et al. (2012) Circulating tumor cell detection in advanced non-small cell lung cancer patients by multi-marker QPCR analysis. Lung Cancer 75: 242-247.
- Punnoose EA, Atwal S, Liu W, Raja R, Fine BM, et al. (2012) Evaluation of circulating tumor cells and circulating tumor DNA in non-small cell lung cancer: association with clinical endpoints in a phase II clinical trial of pertuzumab and erlotinib. Clin Cancer Res 18: 2391-2401.
- Zhang Z, Xiao Y, Zhao J, Chen M, Xu Y, Zhong W, et al. (2016) Relationship between circulating tumour cell count and prognosis following chemotherapy in patients with advanced non-small-cell lung cancer. Respirology 21: 519-525.
- Crosbie PAJ, Shah R, Krysiak P, Zhou C, Morris K, Tugwood J, et al. (2016) Circulating Tumor Cells Detected in the Tumor-Draining Pulmonary Vein Are Associated with Disease Recurrence after Surgical Resection of NSCLC. J Thorac Oncol 11:1793-1797.
- Coco S, Alama A, Vanni I, Fontana V, Genova C, et al. (2017) Circulating Cell-Free DNA and Circulating Tumor Cells as Prognostic and Predictive Biomarkers in Advanced Non-Small Cell Lung Cancer Patients Treated with First-Line Chemotherapy. Int J Mol Sci 18: E1035.
- Tong B, Xu Y, Zhao J, Chen M, Xing J, et al. (2017) Prognostic significance of circulating tumor cells in non-small cell lung cancer patients undergoing chemotherapy. Oncotarget 8: 86615-86624.
- Turetta M, Bulfoni M, Brisotto G, Fasola G, Zanello A, Biscontin E, et al. (2018) Assessment of the Mutational Status of NSCLC Using Hypermetabolic Circulating Tumor Cells. Cancers (Basel) 10: E270.
- Sinoquet L, Jacot W, Gauthier L, Pouderoux S, Viala M, et al. (2021) Programmed Cell Death Ligand 1-Expressing Circulating Tumor Cells: A New Prognostic Biomarker in Non-Small Cell Lung Cancer. Clinical Chemistry 67:1503-1512.
- Groot Koerkamp B, Rahbari NN, Büchler MW, Koch M, et al. (2013) Circulating tumor cells and prognosis of patients with resectable colorectal liver metastases or widespread metastatic colorectal cancer: a meta-analysis. Ann Surg Oncol 20:2156-2165.
- Toh JWT, Lim SH, MacKenzie S, de Souza P, Bokey L, et al. (2020) Association between Microsatellite Instability Status and Peri-Operative Release of Circulating Tumour Cells in Colorectal Cancer. Cells 9:425.
- Huang X, Gao P, Song Y, Sun J, Chen X, Zhao J, et al. (2014) Relationship between circulating tumor cells and tumor response in colorectal cancer patients treated with chemotherapy: a meta-analysis. BMC Cancer14: 976.
- Tol J, Koopman M, Miller MC, Tibbe A, Cats A, Creemers GJM, et al. (2010) Circulating tumour cells early predict progression-free and overall survival in advanced colorectal cancer patients treated with chemotherapy and targeted agents. Ann Oncol 21:1006-1012.
- Matsusaka S, Suenaga M, Mishima Y, Kuniyoshi R, Takagi K, et al. (2011) Circulating tumor cells as a surrogate marker for determining response to chemotherapy in Japanese patients with metastatic colorectal cancer. Cancer Sci 102: 1188-1192.
- De Albuquerque A, Kubisch I, Stölzel U, Ernst D, Boese-Landgraf J, et al. (2012) Prognostic and predictive value of circulating tumor cell analysis in colorectal cancer patients. J Transl Med 10: 222.
- Barbazán J, Muinelo-Romay L, Vieito M, Candamio S, Díaz-López A, et al. (2014) A multimarker panel for circulating tumor cells detection predicts patient outcome and therapy response in metastatic colorectal cancer: A panel of CTC markers as a prognostic and predictive tool in mCRC. Int J Cancer 135: 2633-2643.
- Konczalla L, Wöstemeier A, Kemper M, Karstens K-F, Izbicki J, et al. (2020) Clinical Significance of Circulating Tumor Cells in Gastrointestinal Carcinomas. Diagnostics (Basel)10: E192.
- Gazzaniga P, Gianni W, Raimondi C, Gradilone A, Lo Russo G, et al. (2013) Circulating tumor cells in high-risk nonmetastatic colorectal cancer. Tumour Biol 34: 2507-2509.
- Iinuma H, Watanabe T, Mimori K, Adachi M, Hayashi N, et al. (2011) Clinical significance of circulating tumor cells, including cancer stem-like cells, in peripheral blood for recurrence and prognosis in patients with Dukes’ stage B and C colorectal cancer. J Clin Oncol 29:1547–1555.
- Sclafani F, Chau I, Cunningham D, Hahne JC, Vlachogiannis G, et al. (2018) KRAS and BRAF mutations in circulating tumor DNA from locally advanced rectal cancer. Sci Rep 8:1445.
- Buim ME, Fanelli MF, Souza VS, Romero J, Abdallah EA, et al. (2015) Detection of KRAS mutations in circulating tumor cells from patients with metastatic colorectal cancer. Cancer Biology & Therapy 16:1289–1295.
- Harris L, Fritsche H, Mennel R, Norton L, Ravdin P, et al. (2007) American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J Clin Oncol 25: 5287–5312.
- Sun Y-F, Xu Y, Yang X-R, Guo W, Zhang X, et al. (2013) Circulating stem cell-like epithelial cell adhesion molecule-positive tumor cells indicate poor prognosis of hepatocellular carcinoma after curative resection. Hepatology 57:1458–1468.
- Yu H, Ma L, Zhu Y, Li W, Ding L, et al. (2020) Significant diagnostic value of circulating tumor cells in colorectal cancer. Oncol Lett 20:317–325.
- Dizdar L, Fluegen G, Van Dalum G, Honisch E, Neves RP, et al. (2019) Detection of circulating tumor cells in colorectal cancer patients using the GILUPI CellCollector: results from a prospective, single-center study. Mol Oncol 13:1548–1558.
- Pan R-J, Hong H-J, Sun J, Yu C-R, Liu H-S, et al. (2021) Detection and Clinical Value of Circulating Tumor Cells as an Assisted Prognostic Marker in Colorectal Cancer Patients. CMAR 13:4567–4578.
- Baek DH, Kim GH, Song GA, Han IS, Park EY, et al. (2019) Clinical Potential of Circulating Tumor Cells in Colorectal Cancer: A Prospective Study. Clin Transl Gastroenterol 10: e00055.
- Yang C, Shi D, Wang S, Wei C, Zhang C, et al. (2018) Prognostic value of pre- and post-operative circulating tumor cells detection in colorectal cancer patients treated with curative resection: a prospective cohort study based on ISET device. CMAR 10:4135–4144.
- Wang L, Zhou S, Zhang W, Wang J, Wang M, Hu X, et al. Circulating tumor cells as an independent prognostic factor in advanced colorectal cancer: a retrospective study in 121 patients. Int J Colorectal Dis 34: 589–597.
- Yu J, Zhang J, Peng T, Fei Z, Jin L, et al. (2022) Predictive Value of Circulating Tumor Cells in Prognosis of Stage III/IV Colorectal Cancer After Oxaliplatin-based First-line Chemotherapy. In Vivo 36:806–813.
- Xiong B, Shi D, Wang S, Zheng L, Zhang C, et al. (2018) Prognostic value of Mesenchymal Circulating tumor Cells: Dynamic monitoring in patients with colorectal cancer. JCO 36: e24052–e24052.
- Hendricks A, Brandt B, Geisen R, Dall K, Röder C, et al. (2020) Isolation and Enumeration of CTC in Colorectal Cancer Patients: Introduction of a Novel Cell Imaging Approach and Comparison to Cellular and Molecular Detection Techniques. Cancers 12: 2643.
- Souza e Silva V, Chinen L, Abdallah E, Damascena A, Paludo J, et al. (2016) Early detection of poor outcome in patients with metastatic colorectal cancer: tumor kinetics evaluated by circulating tumor cells. OTT 9:7503–7513.
- Cohen SJ, Punt CJA, Iannotti N, Saidman BH, Sabbath KD, et al. (2009) Prognostic significance of circulating tumor cells in patients with metastatic colorectal cancer. Ann Oncol 20:1223–1229.
- Lalmahomed ZS, Mostert B, Onstenk W, Kraan J, Ayez N, et al. (2015) Prognostic value of circulating tumor cells for early recurrence after resection of colorectal liver metastases. Br J Cancer 112:556–561.
- Huang SK, Hoon DSB. (2016) Liquid biopsy utility for the surveillance of cutaneous malignant melanoma patients. Mol Oncol 10: 450–463.
- Paterlini-Brechot P, Benali NL. (2007) Circulating tumor cells (CTC) detection: clinical impact and future directions. Cancer Lett 253:180–204.
- De Souza LM, Robertson BM, Robertson GP. (2017) Future of circulating tumor cells in melanoma clinical and research laboratory settings. Cancer Lett 392:60–70.
- Testori AAE, Chiellino S, van Akkooi ACJ. (2020) Adjuvant Therapy for Melanoma: Past, Current, and Future Developments. Cancers (Basel) 12: E1994.
- Hoshimoto S, Faries MB, Morton DL, Shingai T, Kuo C, et al. (2012) Assessment of prognostic circulating tumor cells in a phase III trial of adjuvant immunotherapy after complete resection of stage IV melanoma. Ann Surg 255: 357–362.
- Kiyohara E, Hata K, Lam S, Hoon DSB, et al. (2014) Circulating tumor cells as prognostic biomarkers in cutaneous melanoma patients. Methods Mol Biol 1102:513–522.
- Mazzini C, Pinzani P, Salvianti F, Scatena C, Paglierani M, et al. (2014) Circulating tumor cells detection and counting in uveal melanomas by a filtration-based method. Cancers (Basel) 6:323–332.
- Kiniwa Y, Nakamura K, Mikoshiba A, Ashida A, Akiyama Y, et al. (2021) Usefulness of monitoring circulating tumor cells as a therapeutic biomarker in melanoma with BRAF mutation. BMC Cancer 21:287.
- Rupp B, Ball H, Wuchu F, Nagrath D, Nagrath S, et al. (2022) Circulating tumor cells in precision medicine: challenges and opportunities. Trends in Pharmacological Sciences. 43:378–391.
- Šamija I, Luka? J, Mari?-Brozi? J, Buljan M, Alajbeg I, et al. (2010) Prognostic value of microphthalmia-associated transcription factor and tyrosinase as markers for circulating tumor cells detection in patients with melanoma. Melanoma Research 20:293–302.
- Terstappen. (2011) Circulating melanoma cells and survival in metastatic melanoma. Int J Oncol [Internet]. [cited 2022 Nov 16];38. Available from: http://www.spandidos-publications.com/ijo/38/3/755
- Gray ES, Reid AL, Bowyer S, Calapre L, Siew K, et al. Circulating Melanoma Cell Subpopulations: Their Heterogeneity and Differential Responses to Treatment. Journal of Investigative Dermatology 135:2040–2048.
- Li J, Fu W, Zhang W, Li P, et al. (2018) High Number of Circulating Tumor Cells Predicts Poor Survival of Cutaneous Melanoma Patients in China. Med Sci Monit 24:324–331.
- Hall CS, Ross M, Bowman Bauldry JB, Upshaw J, Karhade MG, et al. Circulating Tumor Cells in Stage IV Melanoma Patients. Journal of the American College of Surgeons 227:116–124.
- Lucci A, Hall CS, Patel SP, Narendran B, Bauldry JB, et al. (2020) Circulating Tumor Cells and Early Relapse in Node-positive Melanoma. Clinical Cancer Research 26: 1886–1895.
- Lin SY, Chang S-C, Lam S, Irene Ramos R, Tran K, et al. (2020) Prospective Molecular Profiling of Circulating Tumor Cells from Patients with Melanoma Receiving Combinatorial Immunotherapy. Clinical Chemistry 66:169-177.
- Siegel RL, Miller KD, Jemal A (2015) Cancer statistics, 2015. CA Cancer J Clin 65: 5–29.
- Siegel RL, Miller KD, Jemal A (2020) Cancer statistics, 2020. CA A Cancer J Clin 70: 7–30.
- Kulemann B, Pitman MB, Liss AS, Valsangkar N, Fernández-del Castillo C, et al. (2015) Circulating Tumor Cells Found in Patients With Localized and Advanced Pancreatic Cancer. Pancreas 44: 547–550.
- Ankeny JS, Court CM, Hou S, Li Q, Song M, Wu D, et al. (2016) Circulating tumor cells as a biomarker for diagnosis and staging in pancreatic cancer. Br J Cancer 114: 1367-1375.
- Martini V, Timme-Bronsert S, Fichtner-Feigl S, Hoeppner J, Kulemann B, et al. (2019) Circulating Tumor Cells in Pancreatic Cancer: Current Perspectives. Cancers (Basel) 11: E1659.
- Wang X, Hu L, Yang X, Chen F, Xu H, Yu H, et al. (2021) Clinical prognostic value of circulating tumor cells in the treatment of pancreatic cancer with gemcitabine chemotherapy. Exp Ther Med 22: 1140.
- Wang Y, Yu X, Hartmann D, Zhou J (2020) Circulating tumor cells in peripheral blood of pancreatic cancer patients and their prognostic role: a systematic review and meta-analysis. HPB 22: 660–669.
- Okubo K, Uenosono Y, Arigami T, Mataki Y, Matsushita D, Yanagita S, et al. (2017) Clinical impact of circulating tumor cells and therapy response in pancreatic cancer. European Journal of Surgical Oncology EJSO 43: 1050-1055.
- Saxena AK (2022) Disconcordance Between Stem Cell Oct4, Sox2, Sox4 and Epithelial Mesenchymal Transition CK 19, EpCAM Markers in Circulating Tumor Cells - MTHFR C677T Gene Variant Increase Risk Factor in Pancreatic Tumors. Int J Can Med 6 I: 9.
- Soeth E, Grigoleit U, Moellmann B, Röder C, Schniewind B, et al. (2005) Detection of tumor cell dissemination in pancreatic ductal carcinoma patients by CK 20 RT-PCR indicates poor survival. J Cancer Res Clin Oncol 131: 669–676.
- Hoffmann K (2007) Detection of disseminated pancreatic cells by amplification of cytokeratin-19 with quantitative RT-PCR in blood, bone marrow and peritoneal lavage of pancreatic carcinoma patients. WJG 13: 257.
- Kurihara T, Itoi T, Sofuni A, Itokawa F, Tsuchiya T, Tsuji S, et al. (2008) Detection of circulating tumor cells in patients with pancreatic cancer: a preliminary result. J Hepatobiliary Pancreat Surg 15: 189–195.
- Khoja L, Backen A, Sloane R, Menasce L, Ryder D, et al. (2012) A pilot study to explore circulating tumor cells in pancreatic cancer as a novel biomarker. Br J Cancer 106: 508–516.
- Bidard FC, Huguet F, Louvet C, Mineur L, Bouché O, et al. (2013) Circulating tumor cells in locally advanced pancreatic adenocarcinoma: the ancillary CirCe 07 study to the LAP 07 trial. Annals of Oncology 24:2057–2061.
- Bissolati M, Sandri MT, Burtulo G, Zorzino L, Balzano G, et al. (2015) Portal vein-circulating tumor cells predict liver metastases in patients with resectable pancreatic cancer. Tumor Biol 36:99199–6.
- Zhang Y, Wang F, Ning N, Chen Q, Yang Z, et al. (2015) Patterns of circulating tumor cells identified by CEP8, CK and CD45 in pancreatic cancer: CTCs patterns by CEP8, CK and CD45. Int J Cancer 136: 1228–1233.
- Earl J, Garcia-Nieto S, Martinez-Avila JC, Montans J, et al. (2015) Circulating tumor cells (CTC) and KRAS mutant circulating free DNA (cfDNA) detection in peripheral blood as biomarkers in patients diagnosed with exocrine pancreatic cancer. BMC Cancer 15: 797.
- Poruk KE, Valero V, Saunders T, Blackford AL, Griffin JF, et al. (2016) Circulating Tumor Cell Phenotype Predicts Recurrence and Survival in Pancreatic Adenocarcinoma. Annals of Surgery 264: 1073–1081.
- Gao Y, Zhu Y, Zhang Z, Zhang C, Huang X, et al. (2016) Clinical significance of pancreatic circulating tumor cells using combined negative enrichment and immunostaining-fluorescence in situ hybridization. J Exp Clin Cancer Res 35: 66.
- Kulemann B, Rösch S, Seifert S, Timme S, Bronsert P, et al. (2017) Pancreatic cancer: Circulating Tumor Cells and Primary Tumors show Heterogeneous KRAS Mutations. Sci Rep 7: 4510.
- Poruk KE, Blackford AL, Weiss MJ, Cameron JL, He J, et al. (2017) Circulating Tumor Cells Expressing Markers of Tumor-Initiating Cells Predict Poor Survival and Cancer Recurrence in Patients with Pancreatic Ductal Adenocarcinoma. Clinical Cancer Research 23: 2681–2690.
- Gemenetzis G, Groot VP, Yu J, Ding D, Teinor JA, et al. (2018) Circulating Tumor Cells Dynamics in Pancreatic Adenocarcinoma Correlate with Disease Status: Results of the Prospective CLUSTER Study. Annals of Surgery 268: 408–420.
- Obermayr E, Maritschnegg E, Agreiter C, Pecha N, Speiser P, et al. (2018) Efficient leukocyte depletion by a novel microfluidic platform enables the molecular detection and characterization of circulating tumor cells. Oncotarget 9: 812–823.
- Lou E, Vogel RI, Teoh D, Hoostal S, Grad A, et al. (2018) Assessment of Circulating Tumor Cells as a Predictive Biomarker of Histology in Women With Suspected Ovarian Cancer. Laboratory Medicine 49: 134–139.
- Deng Z, Wu S, Wang Y, Shi D. (2022) Circulating tumor cell isolation for cancer diagnosis and prognosis. eBioMedicine 83: 104237.
- Pearl ML, Zhao Q, Yang J, Dong H, Tulley S, et al. (2014) Prognostic analysis of invasive circulating tumor cells (iCTCs) in epithelial ovarian cancer. Gynecol Oncol 134:581–590.
- Po JW, Roohullah A, Lynch D, DeFazio A, Harrison M, et al. (2018) Improved ovarian cancer EMT-CTC isolation by immunomagnetic targeting of epithelial EpCAM and mesenchymal N-cadherin. J Circ Biomark 7: 1849454418782617.
- Guo Y-X, Neoh KH, Chang X-H, Sun Y, Cheng H-Y, et al. (2018) Diagnostic value of HE4+ circulating tumor cells in patients with suspicious ovarian cancer. Oncotarget 9: 7522–7533.
- Nie L, Li F, Huang X, Aguilar ZP, Wang YA, et al. (2018) Folic Acid Targeting for Efficient Isolation and Detection of Ovarian Cancer CTCs from Human Whole Blood Based on Two-Step Binding Strategy. ACS Appl Mater Interfaces 10: 14055–14062.
- Obermayr E, Bednarz-Knoll N, Orsetti B, Weier H-U, Lambrechts S, et al. (2017) Circulating tumor cells: potential markers of minimal residual disease in ovarian cancer? a study of the OVCAD consortium. Oncotarget 8: 106415–106428.
- Rao Q, Zhang Q, Zheng C, Dai W, Zhang B, et al. (2017) Detection of circulating tumor cells in patients with epithelial ovarian cancer by a microfluidic system. Int J Clin Exp Pathol 10: 9599–9606.
- Lee M, Kim EJ, Cho Y, Kim S, Chung HH, et al. (2017) Predictive value of circulating tumor cells (CTCs) captured by microfluidic device in patients with epithelial ovarian cancer. Gynecol Oncol 145: 361–365.
- Suh DH, Kim M, Choi JY, Bu J, Kang Y-T, et al. (2017) Circulating tumor cells in the differential diagnosis of adnexal masses. Oncotarget 8: 77195–77206.
- Liu W, Nie L, Li F, Aguilar ZP, Xu H, et al. (2016) Folic acid conjugated magnetic iron oxide nanoparticles for nondestructive separation and detection of ovarian cancer cells from whole blood. Biomater Sci 4: 159–166.
- Blassl C, Kuhlmann JD, Webers A, Wimberger P, Fehm T, et al. (2016) Gene expression profiling of single circulating tumor cells in ovarian cancer - Establishment of a multi-marker gene panel. Mol Oncol 10: 1030–1042.
- Chebouti I, Kasimir-Bauer S, Buderath P, Wimberger P, Hauch Set al. (2017) EMT-like circulating tumor cells in ovarian cancer patients are enriched by platinum-based chemotherapy. Oncotarget 8: 48820–48831.
- Kolostova K, Pinkas M, Jakabova A, Pospisilova E, Svobodova P, et al. (2016) Molecular characterization of circulating tumor cells in ovarian cancer. Am J Cancer Res 6: 973–80.
- Kolostova K, Matkowski R, J?dryka M, Soter K, Cegan M, et al. (2015) The added value of circulating tumor cells examination in ovarian cancer staging. Am J Cancer Res 5: 3363–3375.
- Pearl ML, Dong H, Tulley S, Zhao Q, Golightly M, et al. (2015) Treatment monitoring of patients with epithelial ovarian cancer using invasive circulating tumor cells (iCTCs). Gynecol Oncol 137: 229–238.
- Ning N, Zhan T, Zhang Y, Chen Q, Feng F, et al. (2014) Improvement of specific detection of circulating tumor cells using combined CD45 staining and fluorescence in situ hybridization. Clin Chim Acta 433: 69–75.
- Pearl ML, Zhao Q, Yang J, Dong H, Tulley S, et al. (2014) Prognostic analysis of invasive circulating tumor cells (iCTCs) in epithelial ovarian cancer. Gynecol Oncol 134:581–590.
- Kuhlmann JD, Wimberger P, Bankfalvi A, Keller T, Schöler S, et al. (2014) ERCC1-positive circulating tumor cells in the blood of ovarian cancer patients as a predictive biomarker for platinum resistance. Clin Chem 60:1282–1289.
- Obermayr E, Castillo-Tong DC, Pils D, Speiser P, Braicu I, et al. (2013) Molecular characterization of circulating tumor cells in patients with ovarian cancer improves their prognostic significance -- a study of the OVCAD consortium. Gynecol Oncol 128:15–21.
- Aktas B, Kasimir-Bauer S, Heubner M, Kimmig R, Wimberger P, et al. (2011) Molecular profiling and prognostic relevance of circulating tumor cells in the blood of ovarian cancer patients at primary diagnosis and after platinum-based chemotherapy. Int J Gynecol Cancer 21: 822–830.
- Behbakht K, Sill MW, Darcy KM, Rubin SC, Mannel RS, et al. (2011) Phase II trial of the mTOR inhibitor, temsirolimus and evaluation of circulating tumor cells and tumor biomarkers in persistent and recurrent epithelial ovarian and primary peritoneal malignancies: a Gynecologic Oncology Group study. Gynecol Oncol 123:19–26.
- Poveda A, Kaye SB, McCormack R, Wang S, Parekh T, et al. (2011) Circulating tumor cells predict progression free survival and overall survival in patients with relapsed/recurrent advanced ovarian cancer. Gynecol Oncol 122: 567–572.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, et al. (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68: 394–424.
- Llovet JM, Zucman-Rossi J, Pikarsky E, Sangro B, Schwartz M, et al. (2016) Hepatocellular carcinoma. Nat Rev Dis Primers 2: 16018.
- Mann J, Reeves HL, Feldstein AE. (2018) Liquid biopsy for liver diseases. Gut 67: 2204–12.
- Cui K, Ou Y, Shen Y, Li S, Sun Z, et al. (2020) Clinical value of circulating tumor cells for the diagnosis and prognosis of hepatocellular carcinoma (HCC): A systematic review and meta-analysis. Medicine (Baltimore) 99: e22242.
- Winograd P, Hou S, Court CM, Lee Y, Chen P, et al. (2020) Hepatocellular Carcinoma–Circulating Tumor Cells Expressing PD?L1 Are Prognostic and Potentially Associated with Response to Checkpoint Inhibitors. Hepatol Commun 4:1527–1540.
- Saxena AK. (2022) Non-Synonymous Variants of Methylenetetrahydrofolate Reductase C677T Gene Polymorphism showing Discordance with KRAS Mutation in Circulating Tumor Cells of Hepatocellular Carcinoma - A Rare Case Report. COO [Internet].6. Available from: https://clinicsofoncology.com/uploads/IMG_813338.pdf
- Giordano A, Egleston BL, Hajage D, Bland J, Hortobagyi GN, et al. (2013) Establishment and validation of circulating tumor cell-based prognostic nomograms in first-line metastatic breast cancer patients. Clin Cancer Res 19: 1596–1602.
- Lannin DR, Wang S. (2017) Are Small Breast Cancers Good because They Are Small or Small because They Are Good? N Engl J Med 376:2286–2291.
- Ye Y, Li S-L, Wang J-J, Liu B, et al. (2019) The diagnostic value of circulating tumor cells for lung cancer: A systematic review and meta-analysis. Medicine (Baltimore) 98: e14936.
- Yang C, Zhuang W, Hu Y, Zhu L, et al. (2018) Clinical significance of peripheral circulating tumor cell counts in colorectal polyps and non-metastatic colorectal cancer. World J Surg Onc 16:13.
- Abouleila Y, Onidani K, Ali A, Shoji H, Kawai T, et al. (2019) Live single cell mass spectrometry reveals cancer-specific metabolic profiles of circulating tumor cells. Cancer Sci 110: 697–706.
- Shou X, Li Y, Hu W, Ye T, Wang G, et al. (2019) Six-gene Assay as a new biomarker in the blood of patients with colorectal cancer: establishment and clinical validation. Mol Oncol 13:781–791.
- He Y, Shi J, Shi G, Xu X, Liu Q, et al. (2017) Using the New CellCollector to Capture Circulating Tumor Cells from Blood in Different Groups of Pulmonary Disease: A Cohort Study. Sci Rep 7: 9542.
- Cabel L, Proudhon C, Gortais H, Loirat D, Coussy F, et al. (2017) Circulating tumor cells: clinical validity and utility. Int J Clin Oncol 22: 421–430.
- Lowe AC. Circulating Tumor Cells: Applications in Cytopathology. (2018) Surg Pathol Clin. 11:679–686.
- Bidard F-C, Kiavue N, Ychou M, Cabel L, Stern M-H, Madic J, et al. (2019) Circulating Tumor Cells and Circulating Tumor DNA Detection in Potentially Resectable Metastatic Colorectal Cancer: A Prospective Ancillary Study to the Unicancer Prodige-14 Trial. Cells 8: E516.
- Arrazubi V, Mata E, Antelo ML, Tarifa A, Herrera J, et al. (2019) Circulating Tumor Cells in Patients Undergoing Resection of Colorectal Cancer Liver Metastases. Clinical Utility for Long-Term Outcome: A Prospective Trial. Ann Surg Oncol 26: 2805–2811.
- Wang D, Yang Y, Jin L, Wang J, Zhao X, et al. (2019) Prognostic models based on postoperative circulating tumor cells can predict poor tumor recurrence-free survival in patients with stage II-III colorectal cancer. J Cancer 10:4552–4563.
- Wang W, Wan L, Wu S, Yang J, Zhou Y, Liu F, et al. (2018) Mesenchymal marker and LGR5 expression levels in circulating tumor cells correlate with colorectal cancer prognosis. Cell Oncol 41: 495–504.
- Krebs MG, Sloane R, Priest L, Lancashire L, Hou J-M, et al. (2011) Evaluation and prognostic significance of circulating tumor cells in patients with non-small-cell lung cancer. J Clin Oncol 29:1556–1563.
- Kapeleris J, Kulasinghe A, Warkiani ME, Vela I, Kenny L, et al. (2018) The Prognostic Role of Circulating Tumor Cells (CTCs) in Lung Cancer. Front Oncol 8:311.
- Biel?iková Z, Jakabová A, Pinkas M, Zemanová M, Kološtová K, et al. (2017) Circulating tumor cells: what we know, what do we want to know about them and are they ready to be used in clinics? Am J Transl Res 9:2807–2823.
- Rack B, Schindlbeck C, Jückstock J, Andergassen U, Hepp P, et al. (2014) Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J Natl Cancer Inst 106: dju066.
- Madic J, Kiialainen A, Bidard F-C, Birzele F, Ramey G, et al. (2015) Circulating tumor DNA and circulating tumor cells in metastatic triple negative breast cancer patients. Int J Cancer 136: 2158–2165.
- Cai F, Cen C, Cai L, Falar Luis MA, Biskup E, et al. (2019) Application of Circulation Tumor Cells Detection in Diagnosis and Treatment of Breast Tumors. Rejuvenation Res 22: 498–502.
- Goldkorn A, Ely B, Quinn DI, Tangen CM, Fink LM, et al. (2014) Circulating tumor cell counts are prognostic of overall survival in SWOG S0421: a phase III trial of docetaxel with or without atrasentan for metastatic castration-resistant prostate cancer. J Clin Oncol 32:1136–1142.