Prevalence of Work-Related Musculoskeletal Disorders and Psychosocial Factors Among Teachers of Selected Primary Schools in a Nigerian City
Adesola Ojo Ojoawo PhD1*, Adewale Joseph Adejo BMRPT1
1Department of Medical Rehabilitation, Faculty of Basic Medical Sciences, College of Health Sciences, Obafemi Awolowo University, Ile Ife, Nigeria.
*Corresponding Author:Adesola Ojo Ojoawo, Department of Medical Rehabilitation, Faculty of Basic Medical Sciences, College of Health Sciences, Obafemi Awolowo University, Ile Ife, Nigeria.Tel: 123 0039 68886, Fax: 123 0039 68886
Citation: Adesola Ojo Ojoawo (PhD), Adewale Joseph Adejo (BMRPT) (2023) Prevalence of Work-Related Musculoskeletal Disorders and Psychosocial Factors Among Teachers of Selected Primary Schools in a Nigerian City. Medcina Intern 5: 214.
Received: November 19, 2023; Accepted: December 06, 2023; Published: December 12, 2023.
Abstract
Musculoskeletal disorders (MSD) have been recognized as a considerable problem in the teaching profession and various risk factors have also been documented. The study examined the prevalence and psychosocial factors of work-related MSDs among teachers at selected primary schools in Ile Ife, Osun State, Nigeria.
One hundred and thirty respondents (male=30, female=100) participated in the study. A copy of Nordic and sociodemographic questionnaire was used to assess the MSDs prevalence and psychosocial factors of each of the respondents. The completed questionnaires were collected immediately. The data was analyzed using descriptive and inferential statistics. Alpha level was set at 0.05.
Result showed that the 12 months prevalence of WRMSD was 61 (80.31%) in public ,36 (66.77%) in private schools and 97 (74.6%) combined. The common sites were low back 34(44.7%), wrist/hands 31(40.8%), and ankles 30(39.5%). High prevalence was reported in females 100 (76.9%) and 30(24.6%) of teachers have been prevented from carrying out normal activities due to low back pain. There was significant association between 12 months prevalence and type of school (χ2 =4.592 p= 0.03) and psychosocial factors such as: there is opportunity for promotion (χ2=13.076, p) and senior management attitude is common at work (χ2=14.388, p).
It can be concluded from the study that there was a high prevalence of work-related musculoskeletal disorders among primary schoolteachers more in the public than private with low back pain been prominent. Some psychosocial factors were associated with WRMSDs.
Key Words
Key Words:Low Back Pain, Wrist Pain, Private, Public, Schools.
Introduction
Work is essential in the lives of men and women; nonetheless, it can become a health hazard when it is carried out in an inappropriate way. Some groups of workers, due to occupational characteristics, are more exposed to work related musculoskeletal pain [1]. Teaching profession may be carried out under unfavorable circumstances generating over effort of psycho-physiological functions [2]. Teaching leads to stress, with consequences to physical and mental health and with an impact on professional performance [3]. Social transformations, educational reforms and new teaching models have influenced current conditions of teaching, leading to changes in the profession. Therefore, teachers go from a stable and relatively safe status to a state of instability at work, subsequent to new, precarious and unregulated working modes [3]. In the past decade, different studies described the most prevalent health problems among teachers, in which musculoskeletal disorders, voice problems and psychiatric disorders stand out 1,4,5,6).
Musculoskeletal Disorders (MSDs) are known to be a consequence of repetitive strain, overuse, and work-related disorders. These injuries include a variety of disorders that cause pain in bones, joints, muscles or surrounding structures [7]. The work tasks of schoolteachers often involve significant use of a ‘head down’ posture, such as frequent reading, marking of assignments, and writing on a blackboard [8]. Primary schoolteachers, however, also perform a wide variety of tasks combining basic health childcare and teaching duties, and those that require sustained mechanical load and constant trunk flexion [9]. Nursery schoolteachers have been found to have elevated prevalence of neck, shoulder, arm and low back disorders, and lower-extremity due to activities which require sustained periods of kneeling, stooping, squatting or bending [10].
Schoolteachers, in general, have been demonstrated relative to other occupational groups, to report a high prevalence of MSDs, with prevalence rates of between 40% and 95%. During the course of their work, teachers may be subjected to conditions that cause physical health problems [11,12]. The work of a teacher does not only involve teaching students, but also preparing lessons, assessing students’ work and being involved in extracurricular activities such as sports. Teachers also participate in different school committees. These may cause teachers to suffer adverse mental and physical health issues due to the variety of job functions [13].
There is increasing evidence for an association between psychosocial factors and MSDs among teachers. In research by Chiu et al., the work-related psychosocial factors identified were high psychological job demands, low job control and low social support [14]. The concept of psychological distress is a broad label given to a variety of states and responses related to depression and anxiety [14]. Previous research indicated that there was a high prevalence of psychological distress among schoolteachers [15].
Poor mental health status has been significantly associated with lower back pain among Malay primary schoolteachers, while stress significantly increased the risk of back pain among Filipino teachers by approximately four-fold [16,17]. It has been reported that, the more psychological demands needed for a certain task, the greater the possibility to develop MSDs regardless of the anatomical area [18].
Some theoretical models have proposed that the role of physical and psychosocial factors in the development of MSDs is complex or involves complex relationships [19-21]. However, this study will help to investigate the complexity of prevalence and psychosocial factors of work-related musculoskeletal disorders in selected primary schoolteachers. The objectives of the study were to assess the prevalence of work-related musculoskeletal disorder among primary schoolteachers and evaluate psychosocial factors in association with musculoskeletal disorders among primary schoolteachers.
Material and Method
Respondents
Respondents in this study were teachers in selected public and private primary schools within Ile-Ife.
Inclusion criteria
- Primary schoolteachers that had been employed not less than twelve (12) months.
- Primary schoolteachers that were apparently healthy.
Inclusion Criteria
- Primary schoolteachers that had been involved in road traffic accident in the last twelve (12) months.
- Primary schoolteachers that did not consent to the participation.
- Study design
Cross-sectional research design.
Sampling Technique
A Purposive sampling technique was used in this study: ten schools (5 private and 5 public) were selected randomly among the schools and teachers were selected in each of the private and public schools using stratified sampling.
Sample size calculation
Yamane, formula for sample size determination [22]
where:
n sample size
N= Population which was estimated to be 200 in 4 schools. 50 teachers per school
(e)= margin of error (α)
Therefore 133 respondents were recruited for this study.
Site of the Study
This research was carried out at the Department of Medical Rehabilitation, Obafemi Awolowo University, Ile-Ife.
Instrument
Nordic Musculoskeletal questionnaire was used to obtain information from each respondent. The Nordic musculoskeletal questionnaire is a standardized questionnaire which allows comparison of musculoskeletal disorders affecting nine body sites namely: neck, shoulders, upper back, elbows, low back, wrist/hands, hips/thighs, knees and ankles/feet. The questionnaire was divided into three sections.
Section a: This section was designed to obtain socio-demographic data of the respondents like Sex, Age, Years of stay in the school.
Section b: This was designed to obtain information on work-related musculoskeletal pain. It asked questions like, mode of onset of the pain, duration of the pain, effect of the pain on market activities, activity that brought the pain and site where the pain is felt and using the present pain index (Finch, 1987) to score the pain on a scale of 0-5.
Section c: This was designed to obtain information on work-related musculoskeletal injury, average number time of the injury, and cause of the injury.
Instrumentation
The respondents were required to answer the Work Organization Assessment Questionnaire (WOAQ) [23] that assesses workplace psychosocial hazards. The WOAQ scale contained 28 items. The instrument is a self-report questionnaire with a 4-point Likert type scale response format ranging from 1- Strongly disagree, to 4 – Strongly agree. The values of 1–2-point likerts reflects good fit, less than 3 represents acceptable fit and less than 4 demonstrates adequate fit. The reliability of the WOAQ was 0.93 [24].
Procedure
Ethical approval was obtained from Health Research and Ethics Committee of Institute of Public Health College of Health Sciences, Obafemi Awolowo University Ile-Ife (HREC number – IPHOAU/12/1684). Official permission was requested from the Local Inspectorate office, as well as from each school. In addition, the consent of each teacher was taken before the survey questionnaire is administered. Each respondent was given a copy of a questionnaire that was collected after completion within the same day, but we were unable to retrieve 3 questionnaires.
Data Analysis
The data collected were analyzed, organized and processed using Statistical Package for Social Sciences (SPSS 23). The statistical analysis of mean, standard deviation, percentage and inferential, statistical of Chi-square method were used to assess the association between psychosocial factors and prevalence of work-related musculoskeletal disorders.
Results
Socio-demographic Characteristics of Respondents.
Figure I: Socio-demographic Characteristics of Respondents.
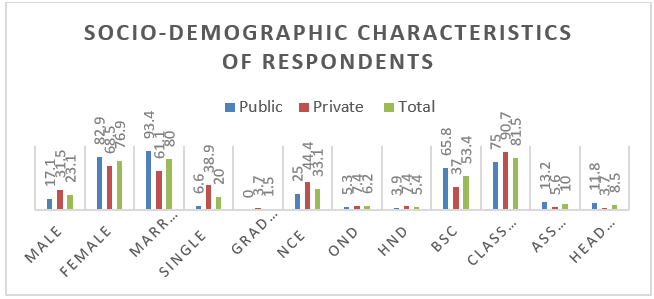
The sociodemographic characteristics of respondent was shown in figure 1, There were 30 (23.1%) male and 100 (76.9%) female from both public and private schools. 104 (80%) of respondents were married, 26 (20%) respondents were single. The table shows two (1.5%) respondents with Grade II, 43 (33.1%) respondents with NCE and 70 (53.8%) respondents with BSc from both public and private schools. The table also shows 106 (81.5%) respondents class teacher, 13 (10.0%) respondents assistant head teacher and 11 (8.5%) respondents head teacher.
Twelve- and seven-days Prevalence of Musculoskeletal Disorder in both private and public primary schools.
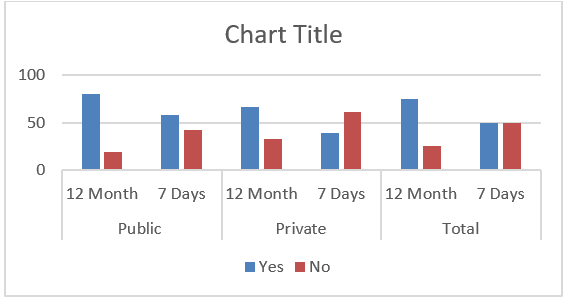
Presented in figure II is prevalence of musculoskeletal pain among respondents. Considering 12 months prevalence, 61 (80.3%) respondents reported pain in public schools while 18 (33.3%) respondents had pain in private schools the prevalence in the total respondents was 97 (74.6%). Regarding 7 days prevalent, 44 (57.9%), 22 (38.9%) and 65 (50%) respondents reported pain in public and private and combining both private and public primary schools respectively, Fig II.
Figure II: Prevalence of musculoskeletal pain among respondents.
12 months prevalence of musculoskeletal pain at different parts of the body
Table 1 shows the percentage distribution of respondents who have had pain in the last twelve months at various sites of the body. The most reported site with pain was low back 34 (44.7%) followed by 31 (40.8%) respondents with pain in the wrists/hand and 20 (26.3%) respondents reported least pain at the shoulder in public primary schools. 16 (29.6%) respondents reported the most site of pain in the lower back and ankles/feet while 9 (16.7%) respondents reported the least pain in the elbows in private schools.
Table 1: 12 months prevalence of musculoskeletal pain at different parts of the body.
|
Variables |
Public |
Private |
Total |
|
|
f % |
f % |
f % |
|
Have you at any time during the last 12 months had trouble such as (ache pain, discomfort, numbness) in |
|||
|
Neck: Yes |
25 (32.9) |
14 (25.9) |
39 (30.0) |
|
No |
51 (67.1) |
40 (74.1) |
91 (70.0) |
|
Shoulder: Yes |
20 (26.3) |
15 (27.8) |
35 (26.9) |
|
No |
55 (72.4) |
39 (72.2) |
94 (72.3) |
|
Upper Back: Yes |
25 (32.9) |
11 (20.4) |
36 (27.7) |
|
No |
51 (67.1) |
43 (79.6) |
94 (72.3) |
|
Elbow: Yes |
16 (21.1) |
9 (16.7) |
25 (19.2) |
|
No |
60 (78.9) |
45 (83.3) |
105 (80.8) |
|
Hands: Yes |
31 (40.8) |
13 (24.1) |
44 (33.8) |
|
No |
45 (59.2) |
41 (75.9) |
86 (66.2) |
|
Low back: Yes |
34 (44.7) |
16 (29.6) |
50 (38.5) |
|
No |
42 (55.3) |
38 (70.4) |
80 (61.5) |
|
Hip/Thigh: Yes |
24 (31.6) |
11 (20.4) |
35 (26.9) |
|
No |
52 (68.4) |
43 (79.6) |
95 (73.1) |
|
Knee: Yes |
28 (36.8) |
15 (27.8) |
43 (33.1) |
|
No |
48 (63.2) |
39 (72.2) |
87 (66.9) |
|
Ankle: Yes |
30 (39.5) |
16 (29.6) |
46 (35.4) |
|
No |
46 (60.5) |
38 (70.4) |
84 (64.6) |
Table 2 shows the percentage distribution of respondents who have pain in the last 7 days at various sites of the body. The most reported site with pain was low back 25 (32.9%) followed by 22 (28.9%) respondents with pain in the wrists/hand and ankles also 14 (18.4%) respondents reported least pain at the neck in public primary schools. 12 (22.2%) respondents reported the most site of pain in the lower back while 5 (9.3%) respondents reported the least pain in the elbows, upper back and hips in private schools.
Table 2: 7 days prevalence of musculoskeletal pain at the neck, shoulder and elbow, wrist, lower back, hips, knees and ankles (N=130).
|
Variables |
Public |
Private |
Total |
|
|
f % |
f % |
f % |
|
Have you at any time during the last 12 months had trouble such as (ache pain, discomfort, numbness) in |
|||
|
Neck: Yes |
14 (18.4) |
10 (18.5) |
24(18.5) |
|
No |
62(80.3) |
44 (81.4) |
106 (81.5) |
|
Shoulder: Yes |
19 (25.0) |
5 (9.3) |
24 (18.5) |
|
No |
57 (75.0) |
49 (90.7) |
106 (81.5) |
|
Upper Back: Yes |
20 (26.3) |
5 (9.3) |
25 (19.2) |
|
No |
56 (73.7) |
49 (90.7) |
105 (80.8) |
|
Elbow: Yes |
7 (9.2) |
6 (11.1) |
13 (10.0) |
|
No |
69 (90.8) |
48 (88.9) |
117(90.0) |
|
Hands: Yes |
22 (28.9) |
8 (14.8) |
30 (23.1) |
|
No |
54 (71.1) |
46 (85.2) |
100(76.9) |
|
Low back: Yes |
25 (32.9) |
12 (22.2) |
37 (28.5) |
|
No |
51 (67.1) |
42 (77.8) |
93 (71.5) |
|
Hip/Thigh: Yes |
15 (19.7) |
5 (9.3) |
20 (15.4) |
|
No |
61 (80.3) |
49 (90.7) |
110 (84.6) |
|
Knee: Yes |
21(27.6) |
10 (18.5) |
31 (23.8) |
|
No |
55(72.4) |
44 (81.5) |
99 (76.2) |
|
Ankle: Yes |
22 (39.5) |
8 (14.8) |
30 (23.1) |
|
No |
54 (71.1) |
46 (85.2) |
100 (76.9) |
Table 3 shows the percentage distribution of respondents who have been prevented from carrying out normal activities due to pain at various sites of the body in the last twelve months. Eighteen (23.7%) respondents reported the most prevalent of knee and lower back pains preventing them from carrying out normal activities in public schools while fourteen (25.9%) respondents reported the most prevalent of knee pains preventing them from carrying out normal activities in private schools.
Table 3: Percentage distribution of respondents who have been prevented from carrying out normal activities due to pain at various sites of the body (N=130).
|
Variables |
Public |
Private |
Total |
|
|
f % |
f % |
f % |
|
During the last 12 months have you been prevented from carrying out normal activities: |
|||
|
Neck: Yes |
16 (21.1) |
11 (20.4) |
27 (20.8) |
|
No |
60 (78.9) |
43 (79.6) |
103 (79.2) |
|
Shoulder: Yes |
12 (15.8) |
9 (16.7) |
21 (16.2) |
|
No |
64 (84.2) |
45 (83.3) |
109 (83.8) |
|
Upper Back: Yes |
14 (18.4) |
10 (18.5) |
24 (18.5) |
|
No |
62 (81.6) |
44 (81.5) |
106 (89.2) |
|
Elbow: Yes |
6 (7.9) |
8 (14.8) |
14 (10.8) |
|
No |
70 (92.1) |
46 (85.2) |
116(89.2) |
|
Hands: Yes |
7 (9.2) |
8 (14.8) |
30 (23.1) |
|
No |
69 (90.8) |
46 (85.2) |
100(76.9) |
|
Low back: Yes |
18 (23.7) |
12 (22.2) |
30 (23.1) |
|
No |
58 (76.3) |
42 (77.8) |
100 (76.9) |
|
Hip/Thigh: Yes |
10 (13.2) |
7 (13.0) |
17 (13.1) |
|
No |
66 (86.8) |
47 (87.0) |
100 (86.9) |
|
Knee: Yes |
18 (23.7) |
14 (25.9) |
32 (24.6) |
|
No |
58 (76.3) |
40 (74.1) |
98 (75.4) |
|
Ankle: Yes |
15 (19.7) |
9 (16.7) |
30 (18.5) |
|
No |
61 (80.3) |
45 (83.3) |
100 (81.5) |
Table 4 shows the association between socio-demographic variables and prevalent of pain that there was a significant association (P<0.05) between prevalence of pain and type of school.
Table 4: Association between socio-demographic variables and seven days prevalence of WRMSD.
|
Variables |
Yes
|
No
|
X2 |
P Value |
|
|
f % |
f % |
|
|
|
Types of School |
|
|
|
|
|
Public |
44 (67.69) |
32 (49.23) |
4.592 | 0.032 |
|
Private |
21(32.31) |
33 (50.77) |
|
|
Presented in table 5 is the association between psychosocial factors and prevalence of musculoskeletal pain in the last 12 months. There was no significant association (P>0.05) between prevalence of musculoskeletal pain and each of psychosocial factors; I am working in a conducive environment (χ2 =2.522) and I am expose to physical danger at work (χ2 =4.696). However, there was a significant association (P<0.05) between prevalence of musculoskeletal pain and each of psychosocial factors; Senior-management attitudes is common at work (χ2 =14.388) and there is opportunity for promotion (χ2 =8.768) in the last 12 months.
Table 5: Association between psychosocial factors and prevalence of 12 months of WRMSD N=130.
|
Variables |
Yes |
No |
X2 |
P Value |
|
|
f % |
f % |
|
|
|
I am working in a conducive environment |
|
|
||
|
SA |
31 (31.96) |
14 (42.42) |
|
|
|
AG |
54 (55.67) |
17 (51.52) |
2.522 | 0.471 |
|
DG |
10 (10.31) |
2 (6.06) |
|
|
|
SD |
2 (2.06) |
0 (0) |
|
|
|
I am expose to physical danger at work |
|
|
||
|
SA |
7 (7.22) |
1 (3.03) |
|
|
|
AG |
19 (19.59) |
4 (12.12) |
4.696 | 0.191 |
|
DG |
48 (49.48) |
14 (42.42) |
|
|
|
SD |
23 (23.71) |
14 (42.42) |
|
|
|
Senior management attitudes is common at work |
|
|
||
|
SA |
15 (15.46) |
1 (3.03) |
|
|
|
AG |
53 (54.64) |
12 (36.36) |
|
|
|
DG |
25 (25.77) |
13 (39.39) |
14.388 | 0.002 |
|
SD |
4 (4.12) |
7 (21.21) |
|
|
|
Senior management attitudes is common at work |
|
|
||
|
SA |
35 (36.08) |
1 (3.03) |
|
|
|
AG |
53 (54.64) |
12 (36.36) |
14.388 | 0.002 |
|
DG |
25 (25.77) |
13 (39.39) |
|
|
|
SD |
4 (4.12) |
7 (21.21) |
|
|
|
There is opportunity for promotion |
|
|
||
|
SA |
35 (36.08) |
4 (12.12) |
|
|
|
AG |
47 (48.45) |
19 (57.58) |
8.768 | 0.002 |
|
DG |
11 (11.34) |
8 (24.24) |
|
|
|
SD |
4 (4.12) |
2 (6.06) |
|
|
Presented in table 6 is the association between psychosocial factors and prevalence of musculoskeletal pain in the last 7 days. There was no significant association (P>0.05) between prevalence of musculoskeletal pain and each of psychosocial factors; I am working in a conducive environment (χ2 =0.327) and I am expose to physical danger at work (χ2 =4.696). However, there was a significant association (P<0.05) between prevalence of musculoskeletal pain and each of psychosocial factors; Impact of work on family/social life is negative (χ2 =17.575) and there is opportunity for promotion (χ2 =13.076) in the last 7 days.
Table 6: Association between psychosocial factors and 7 days Prevalence of WRMSD.
|
Variables |
Yes |
No |
X2 |
P Value |
|
|
f % |
f % |
|
|
|
I am working in a conducive environment |
|
|
||
|
SA |
24 (36.92) |
21 (42.42) |
|
|
|
AG |
34 (52.3) |
37 (56.92) |
0.327 | 0.957 |
|
DG |
6 (19.23) |
6 (19.23) |
|
|
|
SD |
1(1.54) |
1 (1.54) |
|
|
|
I am expose to physical danger at work |
|
|
||
|
SA |
7 (10.77) |
1 (1.54) |
|
|
|
AG |
10 (15.38) |
13 (20.0) |
5.698 | 0.127 |
|
DG |
31 (47.69) |
31 (47.69) |
|
|
|
SD |
17 (26.15) |
20 (30.77) |
|
|
|
Senior management attitudes is common at work |
|
|
||
|
SA |
11 (16.92) |
0 (0) |
|
|
|
AG |
14 (21.54) |
13 (20.0) |
|
|
|
DG |
28 (43.08) |
32 (49.23) |
17.575 | 0.001 |
|
SD |
12 (18.46) |
20 (30.77) |
|
|
|
Impact of work on family/social life is negative |
|
|
||
|
SA |
28 (43.08) |
11 (16.92) |
|
|
|
AG |
29 (44.62) |
37 (56.92) |
14.388 | 0.002 |
|
DG |
5 (7.69) |
14 (21.54) |
|
|
|
SD |
3 (4.62) |
3 (4.62) |
|
|
|
There is opportunity for promotion |
|
|
||
|
SA |
35 (36.08) |
4 (12.12) |
|
|
|
AG |
47 (48.45) |
19 (57.58) |
13.076 | 0.004 |
|
DG |
11 (11.34) |
8 (24.24) |
|
|
|
SD |
4 (4.12) |
2 (6.06) |
|
|
Discussion
This study was carried out to assess the prevalence and psychosocial factors of work-related musculoskeletal disorders among teachers at selected primary schools in Ile-Ife, Osun State, Nigeria. The result observed that the age of respondents especially in public primary schools were more than 40 years old while those in private primary schools were just above 30 years old. This shows that teachers in public primary schools may be older than teachers in private primary schools. This may predispose them to some musculoskeletal injuries because as people are aging the tendency to develop musculoskeletal injuries or pain increases. The findings corroborated the work of Cardoso et al., where it was found that teachers aged 40 years or over were more likely to report MSKD of different body sites [12]. It was also observed that, with respect to working experience, most of the respondents in the public primary schools have working experience closer to 20 years whereas those in private primary schools were less than 10 years. This indicated that there can be repetitive injuries based on prolonged number of years in the services. The finding was similar to Krishnan et al., (2021) that the longer the exposure time to occupational risk factors, the higher the chance of getting job related disorders.
Considering the socio-demographic variables of the respondents there were more female teachers in both private and public primary schools. This may indicate that there are more female teachers in teaching professions. Why females are more among teachers may be due to the fact that teachers spend less hours away from home. This observation was also noted by Ammermueller and Dolton [26]. It was found from this study that a larger percentage of public primary schoolteachers had higher degree than private primary schoolteachers this is an advantage to public schoolteachers because they appeared to be more qualified than private schoolteachers. This may be because private primary schools may not have enough money to employ graduate teachers.
From the study, it was observed that there were more class teachers in both public and private primary schools. This is because classroom teachers primarily focus on the planning, preparation and teaching of programs to achieve specific student outcomes. There were far more head teachers in public primary schools than private primary schools this maybe because there were more higher qualification teachers in public primary schools than private primary schools which were found in this study. With respect to psychosocial variables, teachers were agreed in both public and private primary schools with most of the variables like my workload rating is high and there is impact of family/social on my work. This is similar to that of Bayen et al., who reported that having stress among Ethiopian teachers was found to be a risk factor for lower back pain [18]. These associations may occur in that teachers work in stressful conditions with large classes, lack of educational resources and limited reward for their work [12].
It was found from this study that public and private primary schoolteachers disagreed or were unsatisfied with psychosocial variables such as the equipment/IT used at work is new and impact of work on family/social life negative. This was in line with the study of Chinese Secondary Schoolteachers found a positive association between high workload, low colleague support, high job stress, low job satisfaction and neck pain [27]. The study revealed that the 12 months and 7 days prevalence of pain among public primary schoolteachers were more than 12 months and 7 days prevalence of pain among private primary schoolteachers. The reason deduced to this may be because teachers in the public primary schools are older than teachers in private primary schools and also the working experience of teachers in public school are more than teachers in private school. More so, it has been observed that many public schoolteachers are posted to long distance between their place of work and house which may cumulate into sustaining musculoskeletal pain. This corroborated the work of Cardoso et al., and Zhang et al., where it was found that teachers aged 40 years or over were more likely to report MSD of different body sites and that the longer the exposure time to occupational risk factors, the higher the chance of getting job related disorders [12,27].
The study informed that there was 12 months and 7 days highest prevalence of low back pain among public and private primary schoolteachers, but the prevalence was higher among the public than private. This inferred that teachers task involve prolong sitting for marking attendance, assignments and forming notes and this position which can precipitate low back pain. The findings were similar to the study conducted in Philippines and Brazil, 53.3% of secondary schoolteachers [17], and 41.1% of primary and secondary schoolteachers [12] have reported back pain, respectively. Parallels can be drawn to other studies where 40.4% of Malay teachers [16] and 40% of Chinese primary schoolteachers also reported back pain in the 12 months prior to the study [28). In France, 34.8% of schoolteachers had experienced back pain in the previous six months [29]. However, in the previous study by Ojoawo et al; among secondary schoolteachers’ shoulders was found to be the highest prevalent which is in contrary to our findings [30]. The contrary may be because secondary school teacher’s activity involves more of writing on the board, they don’t station in a class rather they move around since they have their staff rooms while primary schoolteachers’ activity involves prolong sitting to assist in writing with the hands of the students and they are station in a class to monitor their students.
The wrists/hand were found to have 12 months and 7 days second highest prevalence of WRMSDs among public and private schools. This association may occur due to constant writing on the chalkboard, carrying of students and regular writing of forming notes. Though, the prevalence was higher in public than private. This was relatively better than what has been reported in similar studies in which wrists pain has been reported low. Upper limb pain was reported by 23.7% of Brazilian schoolteachers [12]. In a Chinese study of secondary schoolteachers, 35.8% reported life-long upper limb pain [8]. Only 8% of schoolteachers in Turkey reported elbow pain [15]; however, a total of 43.9% of primary and secondary schoolteachers in Hong Kong reported MSDs in the arm during the previous month [31]. Wrist pain was a symptom reported by only 13% of the Turkish schoolteachers [32].
From this study, the Ankles was found to be the third most affected anatomical site by WRMSDs in the 12months and 7 days prevalence among public and private schoolteachers. These can occur due to long distance walking, possession of high heel shoes and also prolong standing. This pattern was similar to few studies which have been investigated on WRMSDs of the lower extremities such as hips, legs, knees, ankles and/or feet among teachers. MSDs in the lower extremities have been reported by 41.1% and 33% of Brazilian schoolteachers [12] and US preschool teachers [9] respectively.
It was observed in this study that knee pain is the most prevalent site of the body preventing them from carrying out normal activities among teachers in both public and private schools. Though, the prevalent is higher in public school than private school. This pattern has been reported among different occupational groups. For example, Lemasters et al, (1998) in a study among union of carpenters in USA. Alghadir et al, (2015) among construction workers in Saudi Arabia found knee to be a high risk of joint for WRMSDs. The high prevalence of knee pain preventing them from carrying out normal activities among teachers can be attributed to work-related activities involving walking around.
It was found from this study that there was a significant association between WRMSDs and types of school. It has been suggested that this finding could be due to higher workload, lager students in classes, aged teachers, poor facilities and poor or delayed payment of salaries from the government in public schools. These findings are consistent with findings in the literature, which mention that having more children corresponds to more time dedicated to taking care of children; possibility of more psychological stress; and need of a higher workload to increase family income (Hsin and Felfe, 2014). Musculoskeletal pain was more frequent in teachers with a 40-hour weekly schedule and who worked on two or more shifts, although not all differences observed were statistically significant. Such characteristics suggest that the long and, probably, intense workday could contribute to the occurrence of the event. Teachers’ overworking has been mentioned in other studies, both for pre-school and college teachers (Silvany, 2000, Delcor, 2004,).
This study informed that there was a significant association between 12 months prevalence of musculoskeletal pain and each of psychosocial factors; senior management attitude is common at work and there is opportunity for promotion. This association may occur because of lack of support from senior teachers to junior teachers. Poor mental health status has been significantly associated with lower back pain among Malay primary schoolteachers (Samad, 2010), while stress significantly increased the risk of back pain among Filipino teachers by approximately four-fold (Atlas, 2007). In a Chinese study of secondary schoolteachers, low colleague support, high anxiety, and high workload were significantly associated with neck pain. In the same study, high workload, very low colleague support and high anxiety were positively correlated with upper limb pain (Chiu, 2007).
It was observed also in this study that there was significant association between 7 days prevalence of WRMSDs and each of psychosocial factors; Impact of work on family/social life is negative and there is opportunity for promotion. Psychosocial factors have been positively associated with MSDs among schoolteachers, and the current review suggests that psychosocial factors such as high workload/demands, high perceived stress level, low social support, low job control, low job satisfaction and monotonous work are most likely associated with MSKD among schoolteachers (Tsuboi, 2002, Chiu, 2007, Samad, 2010). This may occur because teachers often work in stressful conditions with large classes, a lack of educational resources, and limited reward for their work (Cardoso, 2009).
Conclusion
It can be concluded from the study that there was high prevalence of work-related musculoskeletal disorders among both public and private primary schoolteachers with low back pain been the most affected region. The types of school were associated with musculoskeletal disorders. Work Related musculoskeletal disorder was associated with each of some psychosocial factors.
References
- Gasparini SM, Barreto SM, Assunção AA (2006) Prevalência de transtornos mentais comuns em professores da rede municipal de Belo Horizonte, Minas Gerais, Brasil. Cad Saúde Públic 22: 2679-2691.
- Zaragoza JME. (1999) O mal-estar docente a sala de aula e a saúde dos professores. São Paulo: EDUSC.
- Reis EJFB, Araújo TM, Carvalho FM, Barbalho L, Silva MO et al. (2006) Docência e exaustão emocional. Educ Soc 27: 229-253.
- Delcor NS, Araújo TM, Reis EJFB, Porto LA, Carvalho FM, et al. (2004) Condições de trabalho e saúde dos professores da rede particular de ensino de Vitória da Conquista, Bahia, Brasil. Cad Saude Publica 20: 187-196.
- Silvany-Neto MAS, Araújo TM, Dutra FRD, Azi GR, Alves RL, et al. (2000) Condições de trabalho e saúde de professores da rede particular de ensino de Salvador, Bahia. Rev Baiana Saúde Pública 24: 45-56.
- Araújo TM, Sena IP, Viana MA, Araújo EM. Mal-estar docente et al. (2005) avaliação de condições de trabalho e saúde em uma instituição de ensino superior. Rev Baiana Saúde Pública 29: 6-21.
- Suzanne C. O’Connell S, Brenda G et al (2010) Cheever Brunner & Suddarth’s Textbook of Medical-surgical Nursing, Volume110th edition, Lippincott Williams & Wilkins.
- Chiu TT, Lam PK (2007) The prevalence of and risk factors for neck pain and upper limb pain among secondary school teachers in Hong Kong. J Occup Rehabil 17: 19–32.
- Grant KA, Habes DJ, Tepper AL (1995) Work activities and musculoskeletal complaints among preschool workers. Appl Ergon 26: 405-410.
- Pillastrini P, Mugnai R, Bertozzi L, Costi S, Curti S, et al. (2009) Effectiveness of an at-work exercise program in the prevention and management of neck and low back complaints in nursery schoolteachers. Ind Health 47: 349-354.
- Allsop L, Ackland T (2010) The prevalence of playing-related musculoskeletal disorders in relation to piano players’ playing techniques and practising strategies. Music Performance Research 3: 61-78.
- Cardoso JP, De Queiroz Batista Ribeiro I, Maria de Araújo T, Carvalho FM (2009) José Farias Borges dos Reis E. Prevalence of musculoskeletal pain among teachers. Revista Brasileira de Epidemiologia 12: 1-10.
- Chong EY, Chan AH (2010) Subjective health complaints of teachers from primary and secondary schools in Hong Kong. Int J Occup Saf Ergon 16: 23-39.
- Chiu TW, L au KT, Ho CW, Ma MC, Yeung TF, et al. (2006) A study on the prevalence of and risk factors for neck pain in secondary school teachers. Public Health 120: 563-565.
- Korkmaz NC, Cavlak U, Telci EA (2011) Musculoskeletal pain, associated risk factors and coping strategies in schoolteachers. Scientific Research and Essays 6: 649-657.
- Samad NIA, Abdullah H, Moin S, Tamrin SBM, Hashim Z et al. (2010) Prevalence of low back pain and its risk factors among schoolteachers. American Journal of Applied Sciences 7: 634-639.
- Atlas AP, Bondoc RG, Garrovillas RA, Lo RD, Recinto J, et al. (2007) Prevalence of low back pain among public high school teachers in the City of Manila. Philippine. Journal of Allied Health Sciences 2: 34-40.
- Beyen TK, Mengestu MY, Zele YT (2013) Low back pain and associated factors among teachers in Gondar Town, North Gondar, Amhara Region, Ethiopia. Occupational Medicine & Health Affairs; 1(5).
- Davis KG, Heaney CA (2000) The relationship between psychosocial work characteristics and low back pain: underlying methodological issues. Clin Biomech 15: 389–406.
- Eatough EM, Way JD, Chang CH (2012) Understanding the link between psychosocial work stressors and work-related musculoskeletal complaints. Appl Ergon 43: 554–563.
- Karsh BT (2006) Theories of work-related musculoskeletal disorders: implications for ergonomic inventions. Theor Issues Ergon Sci 7: 71–88.
- Yamane, Taro. (1967) Statistics, An Introductory Analysis, 2nd Ed., New York: Harper and Row
- Griffiths A, Cox T, Karanika M, Khan S, Tomas et al. (2006) Work design and management in the manufacturing sector: development and validation of the work organization assessment questionnaire. Occup Environ Med 63: 669–675.
- Maakip I, Keegel T, Oakman J (2017) Predictors of musculoskeletal discomfort: a cross-cultural comparison between Malaysian and Australian office workers. Appl Ergon 60: 52–57.
- Krishnan KS, Raju G, Shawkataly O. (2021). Prevalence of Work-Related Musculoskeletal Disorders: Psychological and Physical Risk Factors. Int J Environ Res Public Health 18: 9361.
- Ammermüller Andreas, Dolton Peter J. (2006) Pupil-teacher gender interaction effects on scholastic outcomes in England and the USA, ZEW Discussion Papers, No. 06-060, Zentrum für Europäische Wirtschaftsforschung (ZEW), Mannheim
- Zhang X, Guo J, Ma L, Xu R, Wang J, et al. (2023) Teacher stress among public primary and secondary schoolteachers in Datong, a city of Shanxi Province, China: association between teacher stress and standardized workload. Int J Occup Med Environ Health 36: 161-176.
- Jin K, Gary S Sorock, Theodore K. (2004). Courtney, Prevalence of low back pain in three occupational groups in Shanghai, People's Republic of China, Journal of Safety Research 35: 23-28.
- Kovess-Masfety V, Sevilla-Dedieu C, Rios-Seidel C, Nerriere E, Chan Chee C et al. Do teachers have more health problems? Results from a French cross-sectional survey. BMC Public Health 6: 101–113.
- Ojoawo A O, Orakwue B C. (2016) Work related musculoskeletal pain among teachers in selected public secondary schools in Ile-Ife, Nigeria. Annals of Biomedical Sciences 15: 125-133.
- Chong EY, Chan AH (2010) Subjective health complaints of teachers from primary and secondary schools in Hong Kong. Int J Occup Saf Ergon 16: 23-39.
- Korkmaz NC, Cavlak U, Telci EA (2011) Musculoskeletal pain, associated risk factors and coping strategies in schoolteachers. Scientific Research and Essays 6: 649-657.
- Lemasters G K, M R Atterbury, A D Booth-Jones, A Bhattacharya, N Ollila-Glenn, et al. (1998) Prevalence of work-related musculoskeletal disorders in active union carpenters. Occup Environ Med 55: 421–427.
- Alghadir Ahmad, Shahnawaz Anwer, (2015) "Prevalence of Musculoskeletal Pain in Construction Workers in Saudi Arabia", The Scientific World Journal Article ID 529873, 5
- Hsin A, Felfe C. (2014) When does time matter? maternal employment, children's time with parents, and child development. Demography 51: 1867-1894.
- Silvany-Neto MAS, Araújo TM, Dutra FRD, Azi GR, Alves RL et al. (2000) Condições de trabalho e saúde de professors.