Evaluation guidelines of male factor in sub fertile couple.
Brinderjeet Kaur1*
1Consultant, Department of Obstetrics and Gynecology, Santokba Durlabhji Memorial Hospital and Research Center, Jaipur, India.
*Corresponding Author:Brinderjeet Kaur, Consultant, Department of Obstetrics and Gynecology, Santokba Durlabhji Memorial Hospital and Research Center, Jaipur, India. Tel: 9829229289, Fax: 9829229289
Citation: Brinderjeet Kaur (2023) Evaluation guidelines of male factor in sub fertile couple. Medcina Intern 5: 212.
Received: October 11, 2023; Accepted: October 20, 2023; Published: October 31, 2023.
Infertility is the inability of sexually active, non-contraception couples to achieve spontaneous pregnancy at one year. Both male and female factors are responsible for infertility where male factor contributes to 40-50 % of causes of infertility in couples. Unfortunately, in developing nation like India with lack of awareness and rampant illiteracy the onus of infertility is on women and are many a times proclaimed ‘barren’. The male infertility refers to abnormal semen parameters and at times can be present with normal semen parameters. Given the high prevalence of male factor in infertile heterosexual couples, a basic medical history and evaluation of the male partner is warranted at the outset. The aim of this review is to guide clinicians with strategies for evaluation of male infertility.
Key Words
Key Words:Infertility, Male Factor, Diagnostic Evaluation.
Infertility examination is suggested for couples who fail to achieve pregnancy over 12 months of unprotected intercourse. An earlier examination is warranted for couples where female age is more than 35 years. (1) The initial evaluation of the male counterpart includes detailed reproductive history and at least one semen analysis. (2) A women’s health specialist may reasonably obtain the male partner’s medical history and order semen analysis. Any abnormality noted warrants referral to a trained specialist or urologist for complete evaluation. (2)
The approach to male infertility evaluation should be done in a step-by-step manner. (Fig-1)
Figure 1: Recommendations for the diagnostic evaluation of male infertility.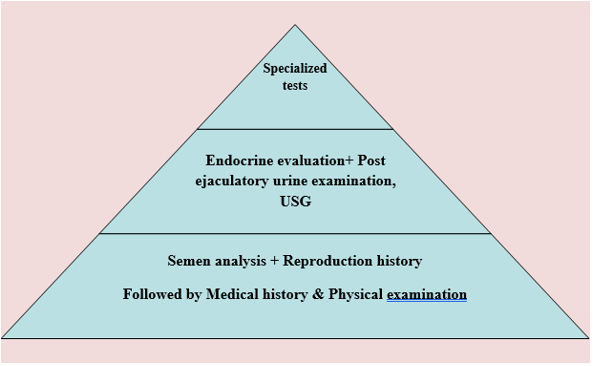
History
The following details the specific key male historical factors to elicit (2) and provide valuable information to decipher the exact cause of couple infertility.
- Coital frequency and timing
- Any evidence of sexual dysfunction, including erectile or ejaculation issues
- Duration of infertility
- Prior infertility
- Childhood illnesses and developmental history
- Systemic medical illnesses.
- Previous surgery e.g cryptorchidism with or without surgery
- Medication use including anabolic steroids and supplement and allergies
- Sexual history and sexually transmitted infections and
- Exposure to gonadal trauma or toxins.
Examination
General Examination, height, weight, BP etc.
- Secoundary sexual characters
- Genital examination of testes (volume, consistency), Epidydymis, Vasa deferentia (prescence, absence), Assess for any abnormalities.
Semen Analysis
The sample should be collected after a minimum of 2 days and maximum of 7 days of sexual abstinence. The man should record time of semen production and deliver the sample to the laboratory within 1 hour of collection. During transport to the laboratory the sample should be kept between 20 – 37-degree C. The semen parameters were measure using recommended method by WHO like volume- weighing or transferring to pipettes or graduated vessel, sperm count by hemocytometer on fixed, dilutes sample, motility at room temperature or 37degree C, morphology by Tygerberg method and vitality by vital dye (Eosin) method.
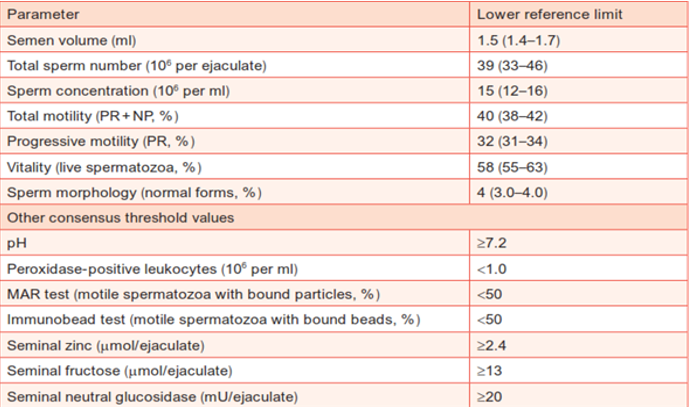
Table -1 shows the normal reference range for seminal fluid parameters. It is worth pointing out that statistical tradition is to take the 2.5th centile from a two-sided reference interval, however for semen parameters one sided reference interval was considered to be appropriate. These semen characteristics are highly variable and are not the sole criteria for fertility as neither those falling with 95% confidence limit guarantee fertility nor those falling below lower limit are all infertile as time to pregnancy is affected by female partners fertility and test interpreted in conjunction with clinical information.
Table 1: Normal reference range of seminal fluid parameters.
Endocrinal Evaluation
They are uncommon causes of male infertility. Hypothalamic pituitary testicular axis abnormalities are well recognized causes of infertility. Endocrinal evaluation is indicated for males with 1) abnormal semen parameters particularly sperm concentration, 2) Impaired sexual function and 3) other clinical findings suggestive of endocrinopathy. Bare minimal hormonal evaluation should include measurement of Serum FSH and Total testosterone (T). In cases of low T less than 300 mg/ml then second morning testing of free testosterone, LH, Prolactin, TSH and Inhibin B is suggested. (Table-2)
Table 2: Basal hormonal levels.
|
Condition |
FSH |
LH |
Testosterone |
|
Normal spermatogenesis |
Normal |
Normal |
Normal |
|
Complete testicular failure |
High |
High |
Normal/ Low |
|
Abnormal spermatogenesis |
High /Normal |
Normal |
Normal |
|
Hypogonadotropic Hypogonadism |
Low |
Low |
Low |
Post Ejaculatory Urinalysis
The test is useful to exclude retrograde ejaculation. It should be performed in men with an ejaculate volume < 1.0 ml but prior to testing one must rule out incomplete collection or short abstinence interval (
Ultrasonography
Trans rectal Ultrasonography reveals dilated seminal vesicles or ejaculatory ducts and or midline cystic prostate structures. Scrotal sonography can rule out varicocele, spermatocele, absent vasa, epididymal indurations and testicular cancer.
Anti sperm antibodies (ASA)
Sperm agglutination or asthenospermia are indications for performing ASA testing. The test relies on the fact that any break in blood –testis barrier and exposure of immune system to larger quantities of sperm antigens or after vasectomy, trauma, torsion, biopsy, orchitis and vasectomy leads to increase in ASA titers.
Sperm DNA Fragmentation (SDF)
Standard semen parameters do not seem to be associated with the risk of pregnancy loss. (3) Routine semen analysis does not take into account the genetic constitution of sperm which is essential for embryo development and implantation. In vitro and in vivo studies have shown elevation of SDF and it negatively affects fertility.(4) and has been proposed as a cause of miscarriage.(5) Current European society for human reproduction and embryology (ESHRE 2017) guidelines recommend sperm DNA fragmentation testing for men whose partners experience recurrent pregnancy loss, unexplained infertility, arrested embryo development, poor blastocyst development, multiple failed IVF, recurrent miscarriage, advanced age, varicocele and toxin drug exposure are some conditions benefitted by sperm fragmentation test.
There are several methods to test SDF, the most commonly used are terminal deoxynucleotidyl transferase d UTP nick end labeling assay, the sperm chromatin dispersion test & the sperm chromatin structure assay (SCSA). SCSA in brief measures susceptibility of sperm DNA to denaturation when it is exposed to heat or acids. Sperms are stained with fluorescent probe that interacts with DNA molecule. The fluorescent signal changes when the DNA is fragmented. These changes are monitored using flow cytometry. DNA fragmentation Index (DFI) is percentage of sperm cells with damaged DNA, normal reference range is less than 15% indicating good to excellent sperm head integrity. DFI more than 50% denotes very poor sperm DNA integrity and the threshold for susceptibility is 25%.
A met analysis of 16 cohort studies involving 2,969 couples found a significant increase in miscarriage in patients with high SDF. (6) Recent cohort study suggest SDF was significantly higher in couples with recurrent pregnancy loss (RPL) compared to a group of fertile men. (7, 8) Therefore, it’s reasonable to offer SDF testing to couples with RPL. Besides, advanced paternal age, many environmental factors, such as smoking, obesity, exogenous heat, and exposure to toxins, have been associated with increased SDF. There are reservations pertaining to routine testing of SDF as a part of workup for RPL (9, 10), however ordering the test could be useful and could help strengthen the decision to pursue lifestyle modifications. (11)
Genetic testing
In extreme cases genetic studies like cystic fibrosis gene (CFTR gene), chromosomal abnormalities like Klinefelter’s syndrome (47, XXY), chromosomal aneuploidy and Y chromosome micro deletion studies are done to ascertain the cause of male infertility.
Prognosis of male infertility
The prognosis depends on the following factors:
- Duration of infertility
- Primary or secondary infertility
- Results of semen analysis
- Age and fertility status of female partner.
Table-3 Causes of Male Infertility.
|
Congenital |
Anorchia |
|
Testicular dysgenesis/cryptorchidism |
|
|
Genetic abnormalities (karyotype, Y-chromosome deletions) |
|
|
Acquired |
Trauma |
|
Testicular torsion |
|
|
Post-inflammatory forms, particularly mumps orchitis |
|
|
Exogenous factors (medications, cytotoxic or anabolic drugs, irradiation, heat) |
|
|
Systemic diseases (liver cirrhosis, renal failure) |
|
|
Testicular tumor |
|
|
Varicocele |
|
|
Surgery that may compromise vascularization of the testes and lead to testicular atrophy |
|
|
Idiopathic |
Unknown etiology |
|
Unknown pathogenesis |
|
|
Known cause |
Mal-descended testes |
|
Varicocele |
|
|
Sperm autoantibodies |
|
|
Testicular tumor |
|
|
Others |
|
|
Idiopathic infertility |
Idiopathic infertility |
|
Hypogonadism |
Klinefelter’s syndrome |
|
XX male |
|
|
Primary hypogonadism of unknown cause |
|
|
Secondary (hypogonadotropic) hypogonadism |
|
|
Kallmann syndrome |
|
|
Idiopathic hypogonadotropic hypogonadism |
|
|
Residual after pituitary surgery |
|
|
Late-onset hypogonadism |
|
|
Constitutional delay of puberty |
|
|
General/systemic disease |
|
|
Cryopreservation due to malignant disease |
Testicular tumor |
|
Azoospermia patients |
|
|
Lymphoma |
|
|
Leukemia |
|
|
Sarcoma |
|
|
Disturbance of erection/ejaculation Obstruction |
Vasectomy |
|
Cystic fibrosis (CBAVD) |
|
|
Others |
Table 4 summarizes the collective evidence and suggested guidelines for various disorders related to male infertility- genetic, obstructive, varicocele, infections and ejaculation disorders. We briefly describe the evidence (in blue) and then the recommendations as suggested by consensus opinion of European guideline (orange).
Table 4: Summary of evidence & recommendations for various disorders of male infertility.
|
Genetic disorders |
|
Spermatogenic damage has higher prevalence of chromosome abnormalities particularly AZF deletions having diagnostic and prognostic value for testicular sperm extraction. Gr/gr deletion has been confirmed as a significant risk factor for impaired sperm production. |
|
Genetic counseling and standard karyotype analysis in all men with damaged spermatogenesis (spermatozoa < 10 million /ml) who are seeking fertility treatment by IVF. For all men with Klinefelter’s syndrome, provide long term endocrine follow up and androgen replacement therapy, if necessary. Do not test for microdeletions in men with obstructive azoospermia (OA) when intracytoplasmic sperm injection (ICSI) is used because spermatogenesis should be normal. Inform men with Yq microdeletion and their partners who wish to proceed with ICSI that microdeletions will be passed to sons, but not to daughters. In men with structural abnormalities of the vas deferens (unilateral or bilateral absence), test the man and his partner for CFTR gene mutations. |
|
Obstructive azoospermia |
|
Obstructive lesions of the seminal tract are frequent in azoospermia or severely oligospermic patients with normal sized testes and normal reproductive hormones. |
|
For azoospermia caused by vassal or epididymal obstruction, perform microsurgical vasovasotomy or tubulovasotomy. |
|
Varicocele |
|
The presence of varicocele in some men is associated with progressive testicular damage from adolescence onwards and a consequent reduction in fertility.Although the treatment of varicocele in adolescents may be effective, there is a significant risk of overtreatment: the majority of boys with a varicocele will have no fertility problems later in life.Varicocele repair was shown to be effective in men with oligospermia. |
|
Treat varicocele in adolescents with progressive failure of testicular development documented by serial clinical examination.Do not treat varicocele in infertile men who have normal semen analysis and in men with a subclinical varicocele but treat those with clinical varicocele, oligospermia and otherwise unexplained infertility. |
|
Cryptorchidism |
|
Cryptorchidism is multifactorial often associated with testicular dysgenesis and is a risk factor for infertility and germ cell tumors.Paternity in men with unilateral cryptorchidism is almost equal to that in men without cryptorchidism.Bilateral cryptorchidism significantly reduces the likelihood of paternity. |
|
Do not use hormonal treatment of cryptorchidism in adults.If undescended testes are corrected in adulthood, perform simultaneous testicular biopsy for detection of intratubular germ cell neoplasia of unclassified type. |
|
Male accessory gland infections |
|
Urethritis and prostatitis are not clearly associated with male infertility.Antibiotic treatment often only eradicates microorganisms; it has no positive effect on inflammatory alterations and cannot reverse functional deficits and anatomical dysfunction and fertility. |
|
Instruct patients with epididymitis that is known or suspected to be caused by N. gonorrhoeae or C. trachomatis to refer their sexual partners for evaluation and treatment. |
|
Disorders of ejaculation |
|
Ejaculation disorders can be treated using a wide range of drugs and physical stimulation (eg vibratory stimulation), with a high level of efficacy.Pharmacotherapy includes either dapoxetine on demand or other off-label antidepressants, and clomipramine that are not amenable to on-demand dosing.men with spinal cord injury, vibrio stimulation and/or electro-ejaculation are effective methods of sperm retrieval. |
|
Offer etiological treatments for ejaculatory disorders before performing sperm collection and ART.Alternatively offer topical anesthetics or tramadol. |
|
Semen cryopreservation |
|
The purpose of sperm cryopreservation is to enable future assisted reproduction techniques procedures.Cryopreservation techniques are not optimal and future efforts are needed to improve the outcome of sperm banking. |
|
Offer cryopreservation of semen to all men who are candidates for chemotherapy, radiation or interventions that might interfere with spermatogenesis or cause ejaculatory disorders.Offer simultaneous sperm cryopreservation if testicular biopsies are performed for fertility diagnosis. |
Conflict of Interest
I hereby declare that I have no conflict of interest.
Sources of Funding
None.
References
- Kumar RM, Shahul S (1998) Role of breast feeding in transmission of hepatitis C virus to infants of HCV –infected mothers. J Hepatol 29: 191-197.
- Diagnostic evaluation of the infertile male: (2015) A committee opinion Practice Committee of the American Society for Reproductive Medicine. Fertil Steril 103: e 18025.
- Hill JA, Abott AF, Politch JA. (1994) Sperm morphology and recurrent abortions. Fertil Sterl 61: 776-778.
- Lewis SE, John Aitken R, Conner SJ, et al. (2013) The impact of sperm DNA damage in assisted conception and beyond: recent advances in diagnosis and treatment. Reprod Biomed Online 27: 325-337.
- Crrell DT, Liu L, Peterson CM, et al. (2003) Sperm DNA fragmentation is increased in couples with unexplained recurrent pregnancy loss. Arch Androl 49: 49-55
- Robinson L, Gallos ID, Conner SJ, et al. (2012) The effect of sperm DNA fragmentation on miscarriage rates: a systematic review and Meta –analysis. Hum Reprod 27: 2908-2917.
- Absalan F, Ghannadi A, Kazerooni M, et al. (2012) Value of sperm chromatin dispersion test in couples with unexplained recurrent abortion. J Assist Reprod Genet 29: 11-14.
- Khadem N, Poorhoseyni A, Jalali M, et al. (2014) Sperm DNA fragmentation in couples with unexplained recurrent spontaneous abortions. Andrologia 46: 126-130.
- Practice Committee of American Society for Reproductive Medicine. (2012) Evaluation and treatment of recurrent pregnancy loss: A committee opinion. Fertil Steril 98: 1103-1111.
- Royal College of Obstetrician and Gynecologists, Scientific Advisory Committee, Guideline No. 17. The Investigation and treatment of couples with recurrent miscarriage, 2011. Accessed January 10, 2017.
- Agarwal A, Majzoub A, Esteves SC, Ko E, Ramaswamy R, et al. (2016) Clinical utility of sperm DNA fragmentation testing: practice recommendations based on clinical scenarios. Transl Androl Urol 5: 935-950.