Results of Maxillo-Mandibular Blockage in the Management of Maxil-Lofacial Fractures in a Country with Limited Resources
Bérété PIJ1*, Djemi EM1, Yapo ARE2, Amenou AD1, Zegbeh NEK1, Ory DMAO1
1Odontostomatology and Maxillofacial Surgery Department of the Bouaké Hospital and University Center (Ivory Coast), West Africa.
2Department of Stomatology and Maxillofacial Surgery of the Hospital and University Center of Treichville (Ivory Coast), West Africa.
*Corresponding Author:Bérété Pornan Issa Jules, Odontostomatology and Maxillofacial Surgery Department of the Bouaké Hospital and University Center (Ivory Coast),West Africa.
Citation: Bérété PIJ, Djemi EM, Yapo ARE, Amenou AD, Zegbeh NEK, et al. (2023)Results of Maxillo-Mandibular Blockage in the Management of Maxil-Lofacial Fractures in a Country with Limited Resources. Medcina Intern 5: 210.
Received: October 07, 2023; Accepted: October 29, 2023; Published: November 06, 2023.
Abstract
Introduction
Maxillomandibular blockade is common practice in our context. The objective of this work was to present the results of maxillomandibular blockade in the management of maxillomandibular fractures.
Material and methods
This was a retrospective study with a descriptive aim carried out over a period of 2 years (January 2021 to December 2022), including the files of patients treated for maxillofacial fractures and treated with maxillomandibular blockade.
Results
The average age of the patients was 30.24 years with the extremes ranging from 4 to 61 years. The male gender was predominant (84.4%) with a sex ratio of 6.40. The etiology was dominated by road traffic accidents in 93% of cases (n=262) mainly due to 2- or 3-wheel vehicles. The socio-professional layer was dominated by motorcycle taxi drivers in 42% of cases (n=119). Mandibular fractures were the most common bone lesions in 45% of cases (n=126). Maxillo-mandibular blocks on vestibular arches were the most performed in 70% of cases (n=196). The average duration of the blockade was 29.5 days ranging from 7 days to 52 days. The treatment was considered good in 99% of cases (n=274). 1 case of dysfunction of the masticator system and 2 cases of mandibular osteitis were noted as complications after a 6-month follow-up.
Conclusion
The maxillo-mandibular blockade allowed the restoration and maintenance of the dental articulation, ensuring good consolidation of fractures and recovery of good masticatory function.
Introduction
Maxillo-mandibular blocking is an orthopedic method which consists of immobilizing the dental arches (maxilla and mandible), in contact with one another to restore the dental articulation to maximum intercuspation [1]. This concept has been known since antiquity [2].
The first writings date from 460 years BC, by Hippocrates using strips of calico glued to the skin near a fracture of the mandible and held on the scalp to obtain occlusion [3]. It is indicated in traumatology maxillofacial in fractures leading to a disorder of the dental articulation, to achieve the reduction and immobilization of the fracture site(s) of the mandible or maxilla in a good dental articulation [1]. This orthopedic process can be carried out by ligation to the steel wire or on vestibular archwires using several methods.
Maxillo-mandibular blocks on ligature appeared during the 19th century and on archwires at the end of the 19th century [4]. It is also used in orthognathic surgery [5].
Maxillomandibular blockade can be used either alone, as an orthopedic treatment during the period of bone consolidation, or as an aid to the reduction and containment of fracture sites before osteosynthesis [1]. In developed countries, the use of osteosynthesis is almost systematic for the treatment of maxillofacial fractures given the high socio-economic level of these countries and the popularization of universal health coverage. On the other hand, in developing countries, the management of maxillofacial fractures remains a challenge for the practitioner because they are very limited in adequate materials for repairing the inherent damage [6]
In Ivory Coast, the lack of public structures for supplying osteosynthesis materials and the low socio-economic status of patients seriously limit access to surgery. Orthopedic treatment then becomes the ultimate solution in the treatment of these fractures. It is commonly used in our practice.
Several recent studies on maxillofacial traumatology have been carried out in our context [7-9]. However, no specific study has focused on maxillomandibular blockade.
It therefore seemed interesting to carry out a study whose objective was to present the results of orthopedic treatment of maxillofacial fractures in an environment with limited resources.
Material and Methods
This was a retrospective study with a descriptive aim carried out in the odontostomatology and maxillofacial surgery department of the Bouaké Hospital and University Center over a period of 02 years from January 2021 to December 2022.
Patients admitted for maxillofacial fractures treated by maxillomandibular blockade were included in our study.
Patients who refused orthopedic treatment, maxillofacial fractures treated surgically, and patients lost to follow-up were not included in our study. A pre-established survey form was used to collect data on the variables studied.
The variables studied were:
-Epidemiological (Frequency, Age, Sex, Etiology, Profession, Consultation time)
-Diagnostics (Type of fractures)
-Therapeutic (Vestibular arch, Ivy ligature, Leblanc ligature, Ern’s ligature)
-Scalable
The outcome evaluation criteria were based on the following clinical parameters:
Restoration of the dental articulation
|
Bad =1 |
Average =2 |
Good =3 |
|
B + CPM + DLI |
B + DLI Or B + CPM |
Dental articulation normal |
B: Béance
CPM: Contact prématuré des molaires
DLI: Déviation de la ligne inter incisive.
Mouth opening
|
Bad =1 |
Average =2 |
Good =3 |
|
< 30 mm |
30-40 mm |
30-40 mm |
Pain
|
Bad =1 |
Average =2 |
Good =3 |
|
Mild Pain |
Slight discomfort while chewing |
No pain |
The score was added with a maximum total of 9 points.
The treatment was judged:
- Good if the score was between 7-9
- Average if the score is between 3-6
- Bad if score less than 3
Results
Frequency
282 maxillofacial fractures collected from 854 maxillofacial traumas.
i.e., a frequency of 33%
Age
The average age was 30.24 years with the extremes ranging from 4 to 61 years.
Sex
There was a male predominance (84.4%).
238 men for 44 women, a sex ratio of 6:40.
Figure 1: Distribution according to age groups.
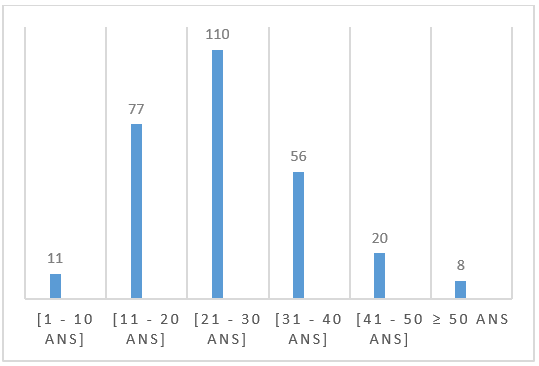
Figure 2: maxillo-mandibular blockage on buccal arches in a patient treated for mandibular fracture.

Etiology
The etiology was dominated by road traffic accidents (93% or n=262) due to 2- or 3-wheel vehicles in 99% of cases.
-Work accident (3% or n=8)
-Domestic accident (2% or n=6)
-Fight (2% or n=6)
Occupation
The socio-professional layer was dominated by motorcycle taxi drivers in 42% of cases (n=119)
Table I: Distribution according to socio-professional layer.
|
Profession |
Workforce |
Percentage (%) |
|
Cultivators |
119 |
42 |
|
Motorcycle taxi drivers |
47 |
17 |
|
Traders |
43 |
15 |
|
Workers |
35 |
12 |
|
Pupils/Students |
26 |
10 |
|
Civil servants |
12 |
4 |
|
Total |
282 |
100 |
Diagnostic Aspects
Mandibular fractures were the most common bone lesions in 45% of cases (n=126) followed by alveolodental fractures in 20% of cases (n=57). All these fractures were simple.
Table II: Distribution according to fracture.
|
Type of fracture |
Numbers |
Percentage (%) |
|
Mandible |
126 |
45 |
|
Alveolodental |
57 |
20 |
|
Maxilla |
48 |
17 |
|
LeFort I + Mandible |
22 |
8 |
|
LeFort I |
18 |
6 |
|
LeFort II |
11 |
4 |
|
Total |
282 |
100 |
Treatment
Maxillo-mandibular blocks on buccal arches were the most performed in (70%=196) of cases followed by Ivy ligature blocks in 12% of cases (n=33)
Table IIb: Distribution according to treatment.
|
Types of blocking |
Numbers |
Percentage (%) |
|
Vestibular arches |
196 |
70 |
|
Ivy method |
33 |
12 |
|
LeBlanc ligature |
27 |
10 |
|
Erns ligature |
15 |
5 |
|
Vestibular arches + internal suspension |
11 |
3 |
|
Total |
282 |
100 |
Maxillomandibular blockade associated with internal ADAMS suspension was considered for the management of Lefort II fractures.
Hygiene-dietary measures were introduced after the blockade:
- Liquid and semi-liquid diet 4 to 6 times a day
- Oral hygiene with a soft brush combined with mouthwash 3 times a day.
Duration of Treatment
The average duration of the blockade was 29.5 days ranging from 7 days to 52 days. Active and passive mechanotherapy was systematic after release.
Evolution
The treatment was considered good in 99% of cases (n=274).
Table III: Distribution according to treatment results.
|
Effective |
Results |
Percentage (%) |
|
Good |
274 |
99 |
|
Medium |
8 |
1 |
|
Bad |
0 |
0 |
On the other hand, 3 types of complications were identified after a 6-month follow-up.
- 1 case of malfunction of the masticatory apparatus
- 2 cases of osteitis (1 right angle osteitis in 1 patient and horizontal branch in another patient)
Discussion
Frequency: The frequency of maxillofacial fractures was 33%. Indeed, maxillofacial fractures are relatively common in our context. This result is consistent with those found in several African series [10-12].
Age and sex: Maxillofacial fractures are observed in all age groups.
In the present study, the average age was 30.24 years and young adult males in the age group between 21-30 years were the most affected. This result was similar to those found by several authors [13 -.15].
This male predominance would probably be explained by the more aggressive nature of male subjects. Finally, it is a population considered mobile and more active. Women are less exposed to risky behaviors [16-18].
The great physical and professional activity at this period of the life of this so-called population, the search for jobs and participation in outdoor activities which are more vulnerable compared to other age groups would explain this high peak in this age group [19-21].
Etiology: The etiology was dominated by road traffic accidents (93% or n=262) due to 2- or 3-wheel vehicles in 99% of cases.
This situation is attributable to the indiscipline of motorcycle users in the city of Bouaké. In addition, it should also be noted the lack of control over these multi-speed machines requiring a driving license, ignorance of the highway code, and lack of knowledge of individual safety measures [22].
Occupation: The socio-professional layer was dominated by farmers followed by motorcycle taxi drivers. This is explained by the fact that farmers considered a less affluent population make a lot of use of 2 or 3 wheeled machines to go about their business. occupations without being able to acquire a 4-wheel vehicle [7].
As for motorcycle taxi drivers, most of them are young people who are not in school or have dropped out of school using 2 or 3 wheeled vehicles for commercial purposes (motorcycle taxis) allowing them to meet their needs. This assertion was shared by Madougou in his study [23].
However, the socio-professional category affected differs from one city to another in the West African sub-region. Indeed, Diallo et al. mainly recorded a population of schoolgirls and students constituting the young population who use motorized bicycles to get to their respective establishments [24].
Type of fractures
The mandibular fracture was the most noted injury.
It is the most common maxillofacial fracture according to the literature. National [3;6], sub-regional [10;25] and even international studies confirm this [26-28]. In fact, the maxillofacial anatomical arrangements place the mandibular level in a prominent position, and therefore expose it more to trauma, hence the clear frequency of fractures at this level based on the experience of the authors and the literature. This opinion is shared by Beogo et al. [11].
Treatment
Blocking on vestibular arches was the most performed among the different types of blocking.
Indeed, it seems more stable than other types of blockages according to the practitioner's experience [29]
Blocking by Ivy ligation was considered mainly in non-displaced fractures [1].
There are also other orthopedic methods such as maxillomandibular blocking using a locking screw. This is a technique described in 1989 [5].
The advantages of this therapeutic option are multiple. Its installation and removal are simpler and quicker than traditional arch wires, while preserving the oral mucosa and the patient's comfort. In addition, it also limits the risk of accident of exposure to blood by reducing handling but risk of nerve or radicular damage [5].
In orthognathic surgery, blocking is also used to immobilize the dental arches according to the planned occlusion, before and during osteosynthesis. Depending on the cases and indications, the blockade will be maintained from a few intraoperative moments to 6 [1].
Evolution
The evolution was good in the majority of cases. On the other hand, the major complication observed was mandibular osteitis. Its occurrence would be attributable to non-compliance with the hygiene measures recommended to the patient.
As for the dysfunction of the manducatory apparatus, it would be due to the prolonged immobilization of the temporomandibular joint for the treatment of a lower subcondylar fracture. Maxillomandibular blockade, despite its importance, has certain disadvantages such as muscle atrophy, reduction in the mineral load of the bone and thinning of the condylar cartilage [30].
Conclusion
Maxillomandibular blockade plays an important role in the management of maxillofacial fractures in our context. It is a treatment of choice given the low socio-economic level of patients. Despite its discomfort, it is less expensive, easy to do and accessible to almost everyone. Its realization requires a pre-therapeutic psychological approach, compliance and above all good teeth of the patient.
References
- Guyot L, Seguin P, Benateau H. Maxillomandibular blockade. Techniques in maxillofacial and facial plastic surgery 105.
- Andrianiaina HD, Rakoto FD, Rakotovao JD, Rakotozafv LF, Randriamanantenasoa VH, et al. (2007) Is intermaxillary blockade obsolete for the treatment of fractures of the mandible in adults? Revue Tropicale de Chirurgie 1: 42-43.
- Rakotondranaivo MJ, Randriamanantena T, Ralahy MF, Rakotoarison RA. (2022) Interest in maxillomandibular blockade alone in the treatment of mandibular fractures. Head and Neck Journal of Madagascar 3: 272-278.
- McGinn JD, Fedok FG (2008) Techniques of maxillary mandibular fixation. Otolaryngol Head Neck Surg 19: 1171-22.
- Graillon N, Gallucci A, Foletti JM, Guyot L, Chossegros C, et al. (2014) Complications due to locking screws. Journal of Stomatology, Maxillofacial Surgery and Oral Surgery 115: 329-330
- Pognon SAB, Biotchane I, Akpovi GD (2013) Management of mandibular fractures. Oral med Oral surgery 19:85-89.
- Zégbeh NEK, Béréte PIJ, SalamI TA, Yapo ARE, Traoré I, et al. (2020) Facial fractures at the Bouaké university hospital center (Ivory Coast): epidemiology and management. Rev Col Odonto-Stomatol Afr Chir Maxillo-fac 27: 66-71.
- Berete PIJ, Zegbeh NEK, Djemi EM, Yapo ARE, Dally YG, et al. (2022) Craniofacial lesions due to public road accidents in Bouake. Health Sci. Dis 23: 114-117.
- Berete PIJ, Zegbeh NEK, Aswan C, Djemi EM, Yapo ARE, et al. (2022) Cranio-Facial Disjunctions: Epidemiological and Clinical Aspects at the Bouake Hospital and University Center in Ivory Coast. Rev Col Odonto-Stomatol Afr Chir Maxillo-fac 29: 45-50.
- Assouan C, Millogo M, Anzouan KE, Nguessan N, Salami A, et al. (2014) Maxillofacial trauma at the Treichville hospital in Abidjan in Ivory Coast. Epidemiological study of 1066 files. Rev Col Odonto-Stomatol Afr Chir Maxillo-fac 21: 31-34.
- Béogo R, Dakouré PWH, Coulibaly TA, Donkor P (2014) Epidemiology of facial fractures: an ana-lysis of fractures of 349 patients. Oral med Oral surgery 20:13-16.
- Bouguila J, Zairi I, Khonsari RH, Jablaoui Y, Hellali H, et al. (2008) Epidemiology of maxillofacial traumatology in Tunis. Rev stomatol Chir maxillofacial 109: 353-357.
- Zounon do Santos AAWC, Kpade AH, Guezo DR, Adjibabi W, Yehouessi-Vignikin B, et al. (2019) Epidemiological-clinical aspects of cranio-facial trauma in public road accidents. Journal Tunisien ENT 42: 42-45.
- Almeimoune A, Mangane MI, Diop Th M, Beye SA, Dembele AS, et al. (2017) Epidemiological and clinical aspects of trauma linked to road traffic accidents involving motorcycle accidents in Bouaké. RAMUR 22: 1.
- Ngaroua, Jérémie Mbo A, Natacha AAM, Yaouba D, Joseph EN, et al. (2016) Fractures due to road accidents at the Ngaoundere Regional Hospital (Cameroon). Health Sci.Dis 17:24-28.
- Muhindo VM, Kalongollumbulumbu M, Kambaleketha J, Katembo SF, Ahua ONA LA, et al. (2018) Support for ATR road traffic accidents in the town of Butembo. Great Lakes Medical Review 9: 1-6.
- Robert S, McCormick, Graham P (2018) The management of facial trauma Surgery Oxford 36:587-594.
- McGreevy J, Stevens KA, Monono ME, et al. (2014) Road traffic injuries in Yaoundé, Cameroon: a hospital-based pilot surveillance study. Injury 45: 1687–1692.
- Omgbwa E, Mbassi NE, Robert SE, Mbella LN, Ebana MC, et al. (2016) Oculo-orbital trauma due to motorcycle accidents in Douala, Cameroon. French Journal of Ophthalmology 39: 596-602.
- Rakotoarivony AE, Rakotoarison RA, Rakotoarimanana FV, Arijaona AN, Rakotoalison SA, et al. (2014) Epidemiology of dental-maxillofacial trauma at CENHOSOA Antananarivo. Oral med Oral surgery 20: 221-226.
- Keita M, Doumbia K, Diani M, Diallo M, Coulibaly M, et al. (2010) Head and neck trauma: 184 cases in Mali. Med Trop 70: 172-174.
- Krah KL, Yao LB, Séry BJLN, Mbra KI, Bénié AC, et al. (2013) Epidemiological data of motorcycle accidents in the surgical emergencies of the Bouaké University Hospital. Rev Int Sc Méd 15:161-164.
- Madougou P, Chigblo A, Tchomtchoua E, Lawson L, Yetognon A, et al. (2016) Incidence and impacts of public road accidents among motorcycle taxi drivers in tropical environments. Journal of Orthopedic and Trauma Surgery 102: 211-214.
- Diallo OR, Diallo AO, Bah AT, Conté AH (2019) Fractures of the middle level of the face at the Conakry University Hospital. Rev Col Odonto Stomato Afr Chir Maxillo Fac 26 :62-67.
- Ba B, Coulibaly DT, Dicko Traoré F, Diallo M, Coulibaly S, et al. (2014) Study of isolated fractures of the mandible at the odontostomatology hospital in Bamako: about 55 cases. Mali Médical 29: 49-52.
- Kelly DE, Harrigan WF (1975) A survey of facial fractures: Bellevue Hospital, 1945-1974. J Oral Surg 33: 146-149.
- Toure G, Meningaud JP, Bertrand JC (2004) Mandible fractures. Paris: Masson, 3rd edition. Medical-surgical encyclopedia. Stomatology 1-9.
- Gola R, Cheynet F (1994) Basis of treatment of mandibular fractures. EMC, Stomatology-Odontology I Paris. 22-070-A-20:1-10.
- Delbet-Dupas C, Pham Dang, Mondié JM, Barthélémy I (2013) Intraoperative maxillomandibular blockade of mandibular fractures: archwires or locking screws? Journal of Stomatology, Maxillofacial Surgery and Oral Surgery 114: 315-321.
- Patrocino LG, Patrocino JA, Borba BHC,Bonatti BDS, Pinto LF, Vieira JV et al. (2005) Mandibular Fracture: analysis of 293 patients treated in the hospital of Clinics, Federal University of Uberlandia. Rev Bras Otorrinolaringol 71: 560-565.
Resume
Introduction
Maxillomandibular blockade is common practice in our context.
The objective of this work was to present the results of maxillomandibular blockade in the management of maxillomandibular fractures.
Material and Methods
This was a retrospective study with a descriptive aim carried out over a period of 2 years (January 2021 to December 2022), including the files of patients treated for maxillofacial fractures and treated with maxillomandibular blockade.
Results
The average age of the patients was 30.24 years with the extremes ranging from 4 to 61 years. The male gender was predominant (84.4%) with a sex ratio of 6.40. The etiology was dominated by road traffic accidents in 93% of cases (n=262) mainly due to 2- or 3-wheel vehicles. The socio-professional layer was dominated by motorcycle taxi drivers in 42% of cases (n=119). Mandibular fractures were the most common bone lesions in 45% of cases (n=126). Maxillo-mandibular blocks on vestibular arches were the most performed in 70% of cases (n=196). The average duration of the blockade was 29.5 days ranging from 7 days to 52 days. The treatment was considered good in 99% of cases (n=274). 1 case of dysfunction of the manducatory apparatus and 2 cases of mandibular osteitis were noted as complications after a 6-month follow-up.
Conclusion
The maxillo-mandibular blockade allowed the restoration and maintenance of the dental articulation, ensuring good consolidation of fractures and recovery of good masticatory function.