Summery Statistics and Methodical Analysis of Neonatal Death at Marie Stopes, Bangladesh
Parvin Rahman1*
1Department of Obstetrics & Gynecology, Associate Professor, Department of Obstetrics & gynecology, CARe Medical College and Hospital, Dhaka, Bangladesh.
*Corresponding Author: Parvin Rahman, Department of Obstetrics & Gynecology, Associate Professor, Department of Obstetrics & gynecology, CARe Medical College and Hospital, Dhaka, Bangladesh, Tel: +880 2-9144459; Fax: +880 2-9144459; E-mail: rahmandrparvin@yahoo.com
Citation: Parvin Rahman(2022) Summery Statistics and Methodical Analysis of Neonatal Death at Marie Stopes, Bangladesh.Int Ginecolgia obstcia2:110.
Copyright: © 2022 Parvin Rahman, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: April 30, 2022; Accepted: May 11, 2022; Published: May 14, 2022
Abstract
Marie Stopes Bangladesh (MSB) is one of the largest provider of high quality and affordable sexual and reproductive health (SRH) services around the country. MSB is active in all 64 districts in Bangladesh, operating with 141 clinics and 15 maternity centers spread around the country. MSB provides service to pregnant women during their pregnancy, women who come in their labor and also women in postnatal period.
Current study is based on a representative 2 year working window of the organization, from June 2014 to March 2016. During this 2 year window, 52689 pregnant women took ANC (Ante-natal Care) service from the different clinics of MSB and 21,499 women gave birth in the different maternity centers. During this period 48 neonatal deaths has occurred. Current study upholds the statistics regarding the neonatal deaths of the chosen working window. This article emphasizes on the Incident Reporting System of MSB and attempts to identify the causes of the Neonatal deaths occurred. Later the article also describes the systematic steps and procedures used to tackle several issues in order to prevent neonatal deaths.
The primary causes for neonatal death was found to be asphyxia & fetal distress (52.08%), complications in post-maturity and post-dated delivery (25%) and neonatal septicemia (10.4%). For each neonatal death, the general procedure that MSB goes through involves forming an investigation team which carefully reviews the history file, takes interviews of the babies’ mothers and relatives and inquire the staffs involved directly or indirectly with the incident. Based on this information the investigation team tries to find out the causes of death. The primary emphasis is given on queries like if there existed any gap in the service provided during the process of labor and delivery, any miscommunication between the service provider and the patient, lacking in counseling patient and patient’s party during antenatal check-up etc. All information about the death are disseminated to all maternity centers so that informative decisions and necessary steps can be taken. If needed, MSB often arranges trainings and workshops for service providers with a goal to equip best to reduce the neonatal deaths. The entire work-process starting from forming the investigation team to ensure proper usage of the gathered information in order to minimize neonatal death can be considered as an effective model suited for developing countries like Bangladesh to deal with such unwanted situations as neonatal deaths and prevent them to the best of human ability.
Keywords
Keywords: Neonatal Deaths, Causes and Solutions, Incident Reporting System, Effective Model.
Background
Marie Stopes International is a non-government organization providing sexual and reproductive health (SRH) services in 37 countries around the world. The organization's core services include family planning, safe abortion and post-abortion care. Also, service on maternal and child health care, safe delivery and pregnancy, diagnosis and treatment of sexually transmitted infections, HIV/AIDS prevention [1]. Bangladesh is a small country in South Asia world's 8th-most populous country with 49.61% women. Marie Stopes Bangladesh (MSB) is one of the largest provider of high quality and affordable sexual and reproductive health (SRH) services of the country. Active in all 64 districts in Bangladesh, operating with 141 clinics and 15 maternity centers spread around the country. MSB Provides service to pregnant women during pregnancy, women who come in labor and women in postnatal period.
Introduction
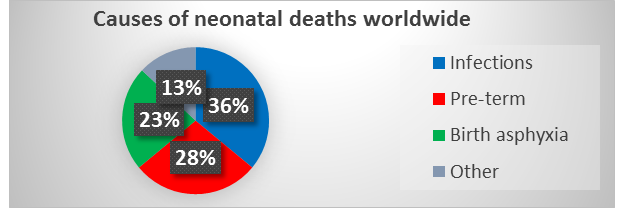
Neonatal death (NND): Death during the first 28 days of life (0-27 days). Neonatal mortality rate (NMR): Number of neonatal deaths per 1000 live births. 130 million infants born each year worldwide among them 4 million die in the first 28 days of life [2-4]. Newborn or neonatal deaths account for 45% of all deaths among children under five. Majority of all neonatal deaths (75%) occur during the first week of life and 25% to 45% occur within the first 24 hours [5]. The three major causes of neonatal deaths worldwide are: (In chart-1) [6]. • Infections which includes sepsis/pneumonia, tetanus and diarrhea (36%).• Pre-term (28%).• Birth asphyxia (23%).
Chart- 1
NMR is a key outcome indicator for newborn care and directly reflects on prenatal, intra-partum & neonatal care.
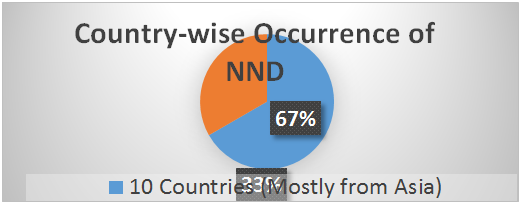
Statistics of NND worldwide: Two-thirds of the world’s neonatal deaths occur in just 10 countries, mostly in Asia [5]. (In chart-2)
Chart- 2
Majority of newborn deaths take place in developing countries where access to health care is low. Skilled health care during pregnancy, childbirth and in the postnatal period prevents complications for mother and newborn, and allows for early detection and management of problems.
Methods and material study
This study upholds the statistics regarding the neonatal deaths at MSB in the chosen working window:
• Emphasizes on the Incident Reporting System of MSB
• Attempts to identify the causes of the Neonatal deaths occurred
• Systematic steps and procedures used to tackle several issues in order to prevent neonatal deaths.
Neonatal deaths are the consequence of events usually associated with poor maternal health and non-availability of care during delivery or immediately after birth. It is important to distinguish the causes of neonatal death; to apply interventions to remove the causes, thereby can prevent neonatal death and further neonatal mortality rate. For that Mariestopes develop a Clinical Incident Reporting & Investigation system to be followed after a NND occurs.
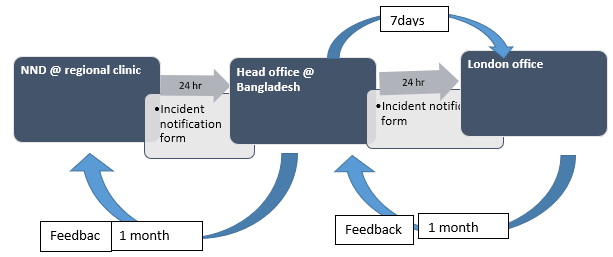
Incident Reporting system: Incident Reporting System is a sequence of systematic actions taken after a NND. Within 24 hours just after death from the center (where death has occurred) service provider/clinic manager have to notice to the head office and from head office to the London office through Incidental Notification Form about the incident. We collected (sealed) the record file/ history file just after neonatal death than we form an investigation team.
Detail procedure of incident investigation System (IIS): Just after incidence collected (sealed) the record file/ history file. After getting the incident report, head office form an investigation team swiftly. Investigation should be started as early as possible (within 3 days) and needs to end with in one week. Team must go to the incident place, review the record file and take interview with mother and relatives of patient. Take interview with all service providers who are involve or present during delivery or during the time of neonatal death face to face and ask them in details about death of the baby. Thus team try to identify the causes of death, try to find out whether there is any gap in service delivery, to find out any gap during the process of labor, to find out any communication gap, gap in counseling patient and patient’s party during antenatal check-up and any knowledge gap of service provider.
After investigation at the clinic, investigation team call a meeting with all staff, and give some feedback, if possible investigation team try to solve the problems immediately in the incident palace if needed. Investigation team try to identify what were the real situations in that time and causes of neonatal death. After getting the all information (direct –indirect causes of neonatal death, service related negligence, gap of service provider etc.) from head office MSB send to the London office within one month. Head office also send scanned copy of all the documents (record file) to the London office. After that from London office they give feedback to the head office within another month. At head office level we call a meeting in each quarter about the incident. Where we discuss: what and where is the problem, how to solve etc. From head office (Dhaka) all information (causes of death, any gap service related etc.) about the death disseminated with others center in our country. After that if needed we take some action: arrange training, refresher training, work shop and make a job aids, protocol etc. for improving knowledge of service provider. See the chart 3.
Purposes of incident systems are:
- To understand the factors that have led to an incident
- To learn from past mistakes and ensure continuous quality improvement.
- To identify risks, and learn from error
- Ultimately this improves the quality of care for our clients as well as maintaining the safety of clients and staffs
Chart- 3: Detail procedure of incident reporting System (IRS).
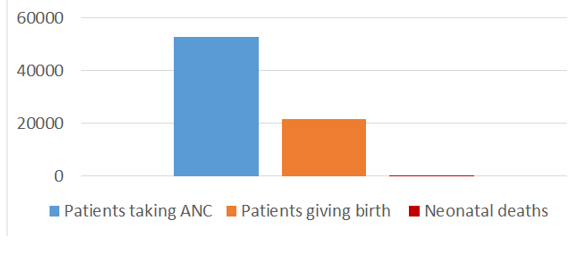
Statistics of NND at MSB in 2 year working window: Current study is based on a representative 2 year working window of MSB, June 2014 - March 2016. During this 2 year window, 52689 pregnant women took ANC (Ante-natal Care) service from the different clinics of MSB and 21,499 women gave birth in the 15 different maternity centers. Out of them 48 neonatal deaths has occurred. Chart -4.
Chart- 4
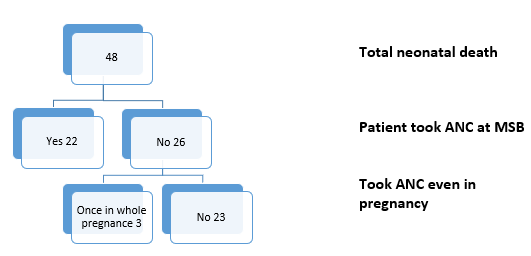
Among 48 neonatal deaths, 26 pregnant mothers did not take any antenatal checkup from our clinic but 3 patient went to the other clinic for checkup once in her whole pregnancy period. See chart-5.
Chart- 5
Among 48 neonatal deaths 31 babies was delivered by caesarean section. Chart (6 & 7)and 17 through vaginal route ( chart-8). Among 31 caesarean sections 13 was done emergency due to fetal distress and 18 caesarean sections had done due to other indications. 18 caesarean sections(C/S) among them 10 was done due to history of previous C/S, 2 was due to breech presentation, 2- due to premature rupture of the membrane, 2- prolonged labor one of them admitted in 2nd stage of labor, 1- due to polyhydramnios, 1 – postdated (6days). Chart- 6,7.
Chart- 6:
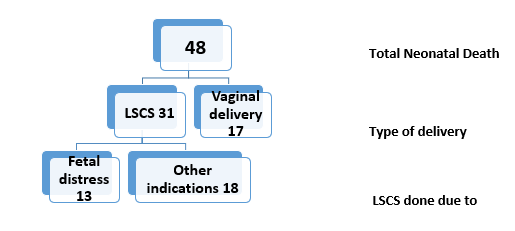
Chart-7: Details of other indications of LSCS.
|
History of previous C/S |
10 |
|
Breech presentation |
2 |
|
Premature rupture of the membrane |
2 (1 LBW, 1 congenital hirschprung) |
|
Polyhydramnios |
1 ( 2.3 kg, congenital heart disease) |
|
Postdated |
1 (6 days, congenital cyanotic heart disease) |
|
Prolonged labor |
2 |
Chart- 8: 17 babies died, delivered through vaginal route
|
Admitted in 2nd stage of labor-7 |
Asphyxiated baby delivered-5 |
Preterm baby-1 |
Big baby-1 |
Cord compression-3 |
|
3 -delivered asphyxiated baby with in few minutes. 2- In prolonged 2nd stage of labor, FHR did not monitor properly. 1- Babydied after coming head arrest in breech delivery. 1- Sudden infantile death (after 8 hours of delivery)
|
FHR not monitor properly.
|
1.9 kg,FHR not monitor properly.
|
4.2 kg shoulder arrest. |
3- 5 times cord around the neck |
Detailed Causes of NND –describe in bellow
|
Causes of death |
Number of death |
|
Congenital anomaly: Cyanotic heart disease 6 Hirschprung disease 1 Turner Syndrome 1
|
8 |
|
Rh incompatibility 1 |
|
|
Cord compression(2,3 even 5 times cord around the neck) |
4 |
|
Prolonged labor: 1st & 2nd stage 1 2nd stage 4 |
|
|
Fetal distress: In Term pregnancy in 2nd stage( late admission) Meconium aspiration syndrome Premature labor 4 Respiratory Syndrome (RDS) |
14 |
|
Septicemia (IUGR, Premature /LBW, term ) |
5 |
|
Postdated & post maturity: ( 6-16 days) 8 Home trail ( Injudicious use of Oxytocin) with Fetal distress 6 Admit in 2nd stage ( Full dilation) with Fetal distress 8 |
|
|
Perinatal asphyxia: (term pregnancy, preterm labor & post term) |
11 |
|
Shoulder arrest ( cord around the neck) |
1 |
|
Head arrest after coming breech delivery |
2 |
|
Ruptured uterus |
1 |
|
Sudden Infantile Death Syndrome |
2 |
Gaps found from IRS & according to that actions were taken which shows in bellow: After reviewing all the record files, 20 of 48 (41.66)% cases were found which had lack of monitoring and poor documentation.
|
Gaps found from incidents
|
Recommendation and action taken for reducing death
|
|
q Poor counseling to the client by the doctors/ counselors/field workers q Poor motivation for hospital delivery, admitted to the clinic in late stage
|
Discussion on ANC counseling strengthening both in field & clinic level Emphasized on Doctor’s workshop |
|
v Admitted in late stage v Lack of awareness of patient and relatives
|
v Discussion on ANC counseling strengthening v both in field & clinic level
|
|
|
|
|
Discussion
Most of the pregnant mother 23 (47. 9 % of NNDs) never goes to the doctor for antenatal checkup. 8 patient (16.7%) came to the hospital in late 2nd stage. Most of the death has occurred due to asphyxia & fetal distress 25 (52.08%). Many patient came in late and asphyxia occurred due to prolonged labor 5 (1st & 2nd stage). Client came in late stage with fetal distress. 8 patients had come to the hospital with postdated & post maturity. Some patient [6] had come after trail of delivery at home. Even after use of Inj. Oxytocin.
One patient had ruptured uterus. The patient was 39+weeks of pregnancy in early labor with H/O of previous C/S with scare tenderness. Due to then political unrest in the country, the C/S was delayed to two hours after admission. If the patient had come earlier and time may be we could have avoided the complication of ruptured uterus and saved the baby.
Conclusion
During the 2 year window, 15 maternity centers of MSB delivered 21499 babies with 48 NND. Primary causes of NND was asphyxia & fetal distress, complication of post maturity & post-dated delivery and neonatal septicemia. Most of the patient never go to the doctor during pregnancy. So need to motivate the patients and family about importance of ANC and identify the high risk patient and motivate them to deliver the baby at hospital. Need to discuss why and when to come to the hospital. Also need proper assessment of risk factor and proper diagnosis the patient. So according to that service provider should manage the case properly. At hospital during giving the service proper assessment and monitoring the process & progress of labor and partograph should be maintained. Should improve skill and strengthen knowledge of service provider, for that purpose need to organize training, workshop and session on labor, partograph and baby management. Thus we can give service and proper manage the patient and as well as to reduce the neonatal death.
References
- https://mariestopes.org/
- Högberg U (2005) The World Health Report 2005: "make every mother and child count" - including Africans. Scand J Public Health33: 409-411. [crossref]
- Lawn JE, Cousens S, Zupan J; Lancet Neonatal Survival Steering Team (2005) 4 million neonatal deaths: when? Where? Why? Lancet 365: 891-900. [crossref]
- http://www.who.int/bulletin/volumes/87/2/08-050963/en/
- Newborns: reducing mortality Fact sheet January 2016.
- WHO (2011) Newborn death and illness ,Updated September.