Clinical and Pathological Characteristics of Breast Cancer in Syria.
Suheil Simaan1*
1 Professor & Fmr Chmn of Surgery, Damascus University.
1Adjunct A.Professor of Surgery, Lebanese American University.
*Corresponding Author: Suheil Simaan MD, FACS.Professor & Fmr Chmn of Surgery, Damascus University.Tel: 00961 79 142135; Fax: 00961 79 142135; E-mail:suheil.simaan@gmail.com
Citation: Suheil Simaan(2023)Clinical and Pathological Characteristics of Breast Cancer in Syria.Cancer Prog Diagn 7: 137.
Received: February 24, 2023; Accepted: February 28, 2023; Published: March 16, 2023.
Introduction
Breast cancer (BC) is the most common cancer among women and accounting for 30 % of all female cancers. The behavior and characteristics of BC in Syria was found not much different than that of the neighboring countries like Lebanon, Jordan and Egypt as far as the low median age of incidence and late presentation is concerned. The behavior of BC was also found quite different than seen in the Western countries.
Methods
This is a retrospective study of two main sets of consecutive breast cancer patients operated by the author. The first study included 393 patients from the years 1996 till 2000. The second study included 665 patients from 2000 till 2008 making a total of 1058 breast cancer patients within a period of 12 years. From the second set, 656 charts were selected because they had adequate information.
Every patient chart was reviewed regarding many aspects i.e., age, size of lesion, status of axillary lymph nodes (LN’s), hormonal receptors, and different ways of treatments. The behavior and characteristics of breast cancer (BC) in Syria was found to be quite particular. According to the Syrian MOH cancer registry based on 8000 consecutive cancer cases, the most common cancers seen and treated were breast, colorectal and lung cancer, followed by leukemia (adult and children) and lymphoma (adult and children). Bladder, stomach and prostate were less common.
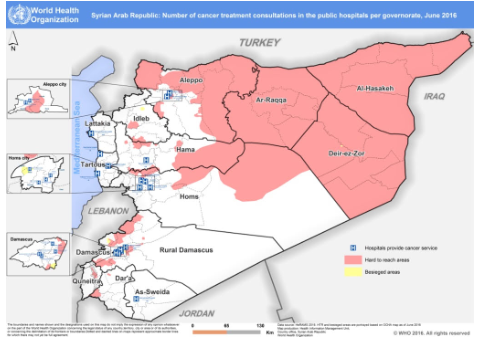
In coordination with WHO Headquarters, WHO Regional Office and the National Committee for Cancer Care, WHO Syria Office has conducted a rapid assessment in 8 hospitals from different governorates between 4th October and 15thNov, 2016 to evaluate the cancer care management in the country.
Discussion and Results
The current global cancer burden in low- and medium income countries is significant, and effective cancer control is limited by inadequate health budget, limited number of cancer treatment facilities and inaccessible diagnostic services and life-saving therapies.
In 2015, 8.8 million cancer deaths occurred worldwide. About 70% of cancer deaths occur in low-income and middle-income countries and this number is likely to increase in the future. It is estimated that cancer kills almost 400,000 people each year in the WHO Eastern Mediterranean Region alone.
Breast Cancer at our MOH in Syria (hospital based) revealed the following:
Frequency of female Breast cancer accounted for 30 % (based on 3000 cases)
Age: Median =49 years
Crude Incidence Rate: 29 per 100,000
Age Standardized Incidence Rate: 43 per 100,000
Histopathology: infiltrating duct carcinoma (70 %)
Unfortunately, due to our present national crisis and civil war resulting into scarcity of resources and disruption of the health system that resulted in limited of human resources, movements of patients, damaged health facilities, and unavailability of health information system. All these factors limited the role of the national cancer registry and its functionality.The last statistics available are dated 2009, and no statistics or reports were produced after that.
According to the top 10 causes of mortality / morbidity in 2009, cancer is ranked 3rd among the 10 leading diseases of mortality and 7th from the 10 leading diseases of morbidity/ disability (Syrian health system profile, 2011).
About 41.5% of women with breast cancer presented with stage III disease, followed by 27.5% presenting to hospitals with stage IV disease. While only 21% presenting in Stage II and 10% presenting in stage I, as shown in the following Figure:
Stage 1. II III IV
10% 21% 42% 27%
87% of death among breast cancer women were due to progressive or relapse in the disease, while the 13 % of the death cases resulted from treatment related toxicities, as shown in the following figure.
13% 87%
The average number of cancer patients seen per month at Damascus University Cancer Center (AlBeiruni Hospital) was 226 patients and the maximum number of patients seen was 500. Albaironi hospital, which is the main referral oncology hospital in the country, is equipped with radio and chemotherapy services and has available oncologists and nurses to provide the required cancer care. About 28% of cancer patients are treated in the mentioned hospital (500 out of 1810).
Map of Syria
According to our MOH Cancer Registry, based on 8000 breast cancer cases collected from several hospitals in Syria, BC accounted for 30 % of female cancers in Syria.
This article with its detailed data is based on my personal studied cases (1058 cases). We have to consider that this group of patients are private and belong to a higher socio-economic class. Average age of incidence was found to be 48 years which is consistent with that figure in neighboring countries like Lebanon, Jordan and Egypt. Those patients below the age of 40 accounted for 20 % of cases (versus 8 % in the western countries). This might be explained by the fact that according to our population pyramid, 82% of our people are under the age of 40.
Lesions below 2 cm in size were 21%, 2-5 cm in size accounted for 55 % Negative axillary LN's increased from 19 % in the first study from 1996-2000 year up to 47% in the next period from year 2000 to 2008. Positive axillary nodes decreased from 81 % to 53 % from 1st study period to the 2nd. Our periodic campaigns in breast cancer awareness are paying off in early detection and better survival. According to the available results from the 2nd study only, Positive ER/PR was 56 %. Positive HER2 accounted for 32%.
Modified Radical Mastectomy (MRM) was done on 72%. Conservative Surgery (CS) accounted for only 20 %.I could not raise this percentage of CS for several reasons: First, stage one cancer was low, second radiotherapy facilities are limited, and many patients' living areas are far in addition to the fact that our patients don't accept local recurrence even though we explain to them that even when local recurrence occurs after CS, salvage mastectomy can be done without affecting overall survival. Conversion from CS to MRM accounted for 8%. Local recurrence after CS was 13 %. One of our patients developed a local recurrence occurred 19 years after MRM. Locally advanced BC was 12%.
This is a picture of LABC of a 27 yr old mother of three, presented to my clinic 2 months ago. She mentioned that one yr earlier she noticed a small lump in her right breast but was considered benign by her physician then neglected by the patient. On preliminary investigations, she showed metastatic lesions in lungs and liver.

This is another picture of LABC of a 55 yr. old lady seen at my clinic one week ago. She mentioned that she felt a left breast small mass 5 years earlier but kept silent about it till one of her daughters noticed both breast lesions on her mother just few days earlier. Chest X-ray and ultrasound to liver were negative.

Due to the present civil war in our country that is still going on for the last seven years, we have not been able to follow up our patients adequately, thus could not give reliable 5-year survival rates.
The detailed data of my personal cases are:
|
|
Distribution according to age |
|
||
|
|
No of cases |
Previous Study (393 cases) |
Present study (656 cases) |
|
|
2nd Decade |
|
2(0.5 %) |
2 (0.3 %) |
|
|
3rd Decade |
|
13 (3 %) |
23 (3.5 %) |
|
|
4th Decade |
|
78 (20 %) |
114 (17%) |
|
|
5th Decade |
|
131 (33%) |
240 (37 %) |
|
|
6th Decade |
|
98 (25%) |
153 (23%) |
|
|
7th Decade |
|
56 (14%) |
97 (15%) |
|
|
8th Decade |
|
16 (4%) |
24 (4%) |
|
|
9th Decade |
|
2 (0.5%) |
3 (0.45%) |
|
|
|
Breast cancer below the age of 40 |
|||
|
|
previous study |
Present Study |
|
|
|
Below 40 |
93 (24%) |
139 (21%) |
|
|
|
40 and above |
300 (76%) |
517 (79%) |
|
|
|
|
|
|
No of children |
|
|
|
Previous study |
Present Study |
(360 cases) |
|
|
Single |
51 (13%) |
|
61 (17%) |
|
|
4 and less |
159 (40%) |
|
150 (42%) |
|
|
> 4 |
86 (22%) |
|
135 (37.5%) |
|
|
No Children |
17 (4% ) |
|
14 (4%) |
|
|
|
Family History |
|
|
|
|
|
Previous Study |
Present Study |
(360 Cases) |
|
|
+ FH |
92 (23%) |
|
77 (21%) |
|
|
- FH |
301 (77%) |
|
283 (79%) |
|
|
Mother |
10 (3%) |
|
7 (2%) |
|
|
Sister |
34 (9%) |
|
30 (8%) |
|
|
P&M Aunt |
20 (5%) |
|
20 (6%) |
|
|
P & M Cousin |
24 (6%) |
|
18 (5%) |
|
|
1 (0.3%) |
|
2 (0.6%) |
|
|
|
Daughter |
3(0.8%) |
|
1 (0.3%) |
|
|
|
|
Size of primary Tumor |
||
|
|
Previous Study |
Present Study |
(464 cases) |
|
|
< 2 cm |
99 (25%) |
|
96 (21%) |
|
|
2 - 5 cm |
166 (42%) |
|
256 (55 %) |
|
|
5 - 10 cm |
41 (10%) |
|
55 (12 %) |
|
|
> 10 cm |
Not Specified |
|
57 (12.3 %) |
|
|
|
|
LN Status |
|
|
|
|
Previous Study |
Present Study |
(464 cases) |
|
|
Neg Nodes |
76 (19%) |
|
220 (47%) |
|
|
317 (81%) |
|
244 (53%) |
|
|
|
1 - 3 Pos nodes |
55 (13%) |
|
76 (16%) |
|
|
3 - 10 Pos nodes |
218 (55%) |
|
132 (28 %) |
|
|
> 10 Pos nodes |
|
37 (8%) |
|
|
|
|
|
Breast Side |
|
|
|
|
|
294 |
|
|
|
Rt |
|
|
293 |
|
|
|
|
Location |
|
|
|
|
|
|
Present Study |
(262 cases) |
|
|
|
UOQ |
145 (55%) |
|
|
|
|
LOQ |
27 (10%) |
|
|
|
|
UIQ |
44 (17%) |
|
|
|
|
LIQ |
20 (8%) |
|
|
|
|
Central |
26 (10%) |
|
|
|
|
Pathology |
|
|
|
|
|
(330 cases |
||
|
351 (89%) |
|
185 (56%) |
|
|
|
6 (1%) |
|
47 (14%) |
|
|
|
Mixed D&L |
|
|
5 (1.5%) |
|
|
4 (1%) |
|
20 (6%) |
|
|
|
11 (3%) |
|
14 (4%) |
|
|
|
Mucinous |
1 (0.2%) |
|
5 (1.5%) |
|
|
Paget |
4 (1%) |
|
10 (3%) |
|
|
DCI |
4 (1%) |
|
30 (9%) |
|
|
LCIS |
|
|
3 (1%) |
|
|
|
6 (2%) |
|
||
|
IBC |
8 (2%) |
|
2 (0.6%) |
|
|
|
|
1 (0.3%) |
|
|
|
|
|
1 (0.3%) |
|
|
|
NHL |
|
|
2 (0.6%) |
|
|
LVI |
|
|
85 (26%) |
|
|
|
|
Receptors |
(412 cases) |
|
|
|
|
|
||
|
ER/PR +/+ |
|
|
230 (56%) |
|
|
- /- |
|
|
140 (34%) |
|
|
+/- |
|
|
20 (5%) |
|
|
-/+ |
|
|
22 (5.4%) |
|
|
|
|
Her 2/neu |
(323 cases) |
|
|
- |
|
|
78 (24%) |
|
|
+ |
|
|
85 (26.3%) |
|
|
++ |
|
|
57 (18%) |
|
|
+++ |
|
|
103 (32%) |
|
|
TNT |
|
|
25 (8%) |
|