Effect of Physical Detraining by the Covid-19 Pandemic on Physiological Parameters in Trained Type 2 Diabetics
Effect of Physical Detraining by the Covid-19 Pandemic on Physiological Parameters in Trained Type 2 Diabetics
Autran José da Silva Júnior1, Lilian Cristiane Gomes1*
1 University Center of the Guaxupé Educational Foundation, Guaxupé, Minas Gerais, Brazil.
*Corresponding Author: Lilian Cristiane Gomes,University Center of the Guaxupé Educational Foundation, Guaxupé, Minas Gerais, Brazil, Tel:+55 35 3551-5267; Fax:+55 35 3551-5696; E-mail: liliancg@unifeg.edu.br; autran@unifeg.edu.br
Citation: Autran José da Silva Júnior, Lilian Cristiane Gomes (2022) Effect of Physical Detraining by the Covid-19 Pandemic on Physiological Parameters in Trained Type 2 Diabetics. Diabetes Cholest metabol6: 142.
Received: December2, 2022; Accepted: December 05, 2022; Published: December15, 2022.
Copyright: © 2022 Lilian Cristiane Gomes, Autran José da Silva Júnior. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction
Acute or chronic exercise is an important non-pharmacological tool for type 2 diabetics, but its interruption characterizes the principle of reversibility and loss of physiological adaptations, glycemic control, and quality of life.
Purpose
To perform anthropometric, cardiovascular, glycemic control and muscle strength assessments in diabetic volunteers after the interruption of physical training, and to compare the results with those obtained before the Covid-19 pandemic.
Methods
16 volunteers, type 2 diabetics, participated in a concurrent training program, three weekly sessions lasting 60 minutes each. Anthropometric, cardiovascular, glycemic control parameters and muscle strength were evaluated during 24 months of training and after an equal period of detraining resulting from the Covid-19 pandemic.
Results
There were significant reductions in cardiovascular parameters (heart rate and blood pressure), blood glucose and muscle strength during the training period, but reversed in the detraining period.
Conclusion
The results demonstrate the deleterious effects of the interruption of physical training and the importance of regular physical exercise/physical activity in glycemic control in patients with type 2 diabetes.
Keywords
Keywords: Physical Detraining, Type 2 Diabetics, Physiological Parameters
Introduction
Among the chronic non-communicable diseases (NCDs), diabetes mellitus (DM) is one of the most worrisome globally, having seen the estimated prevalence of 9.3% in the world population, which represents 463 million people, and approximately the half of them is unaware of their condition. Another aggravating factor is the epidemic projections in a few decades: in 2030, it is estimated that there will be 576 million and, in 2045, 700 million diabetics [1-2]. In Brazil, the situation is no different. In 2013, the country ranked 4th among those with the highest number of cases, about 11.9 million or 6.9% of the population, with 6.5% among men, 7.2% among women, and corresponded to 12 % of total hospitalizations and 15.4% of hospital costs between 2008 and 2010 [3]. In 2011, the Minas Gerais State Health Department (SHD/MG) estimated that 10% of the adult population or approximately 1.3 million are diabetics [4].
In this scenario and considering the scientific evidence on the benefits of education in DM and the regular practice of physical exercises in controlling the disease, we sought to implement in 2017, in a private university center in the interior of Minas Gerais, an educational program for people with type 2 DM (DM2), with the differential of including supervised concurrent physical training sessions.
However, at the end of 2019, the first cases of a respiratory infection caused by a new type of coronavirus, called SARS-CoV-2 by the International Committee on Taxonomy of Viruses [5-6]. Due to the high rate of global infection in early 2020, the World Health Organization (WHO) came to name it as COVID-19, being characterized as a pandemic in March of that same year [7].
To mitigate viral transmission at a time when there were still no effective pharmacological measures, there was a need to immediately impose social distancing [8, 9, 10], causing the interruption of numerous human activities, including the proposed educational program. It is believed that the discontinuation of that program, especially regarding physical training, had a negative impact on anthropometric, cardiovascular, muscle strength and blood glucose parameters. Thus, the objective of the present study was to perform anthropometric, cardiovascular, blood glucose and muscle strength assessments in diabetic volunteers after the interruption of the program, and to compare the results with those obtained prior to the Covid-19 pandemic.
Materials and Methods
Outline and ethical aspects the present study was developed from the matrix project entitled "Evaluation of an educational program for people with type 2 diabetes mellitus, with a focus on the practice of physical activities and foot care", approved by the Research Ethics Committee of the University Center of the Guaxupé Educational Foundation (UNIFEG), opinion No. 2,029,352, of May 3, 2017.
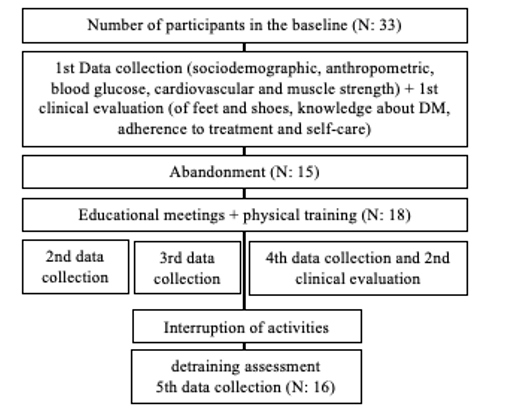
This was a longitudinal and intervention study, with a single comparison group, for the analysis of “before and after” results [11], referring to the educational and physical training program with people with DM2, centered on self-care and concurrent physical training. The representation of all stages of the matrix project and of the present study is shown in (Figure 1). In previous studies [12, 13], arising from the same matrix project, the methodological aspects, described below.
Figure 1: Matrix Project Scheme.
Study Sample
The base population consisted of people with a medical diagnosis of DM2, regardless of the duration of the disease, not hospitalized and in outpatient follow-up. The invitation to the study was carried out in public health services and by the local media. For the selection of the sample, the following inclusion/exclusion criteria were considered:
Inclusion criteria: people of both sexes, aged at least 40 years, sedentary or not very active, without complications in an advanced stage, whose drug treatment included the use of oral antidiabetic drugs (OADs) and/or insulin, and who were able to keep dialogue.
Exclusion criteria: people with DM2 who had at least one of the following conditions were excluded: undergoing hemodialysis, amaurosis, presence of sequelae of stroke/heart failure, previous amputations at any level of the lower limb, injury process or active ulcer in lower limbs, presence of any other disabling complication; use of a wheelchair and/or stretcher; inability to communicate verbally; and participants in a physical training program at another institution.
Thus, the sample was initially composed of 33 people with DM2 who met the inclusion criteria and voluntarily attended the study site. After being instructed on the objectives and procedures of the study, including the need for a medical certificate for the practice of physical exercises, the Free and Informed Consent Term (FICT) was provided for reading and signing. However, 15 participants dropped out of the study due to lack of interest and/or lack of time to attend physical training sessions. The remaining 18 participants attended educational meetings and physical training sessions, as well as follow-up assessments. After the interruption of program activities, due to the Covid-19 pandemic, the detraining evaluation was carried out, in which 16 participants attended, which, therefore, made up the sample of the present study.
Data collect
All evaluations obtained were recorded in individual physical training sheets, with four evaluations carried out before the pandemic enactment, with intervals of approximately six months, and one after, totaling five evaluations. In each of the five assessments, blood glucose variables (glycemic control), anthropometric, cardiovascular and muscle strength were analyzed.
Anthropometric Assessment
Counted measurements of total body weight, waist circumference, and body mass index. Body weight was measured using a Plenna Acqua® 180Kg digital scale with a precision of 100 grams supported on level ground. Total height was measured using a WCS Wood Compact® stadiometer with millimeter precision. Waist circumference was measured using a flexible measuring tape with 1mm precision from the PAMED brand. With the values of body weight and total height it was possible to obtain the body mass index (BMI).
Cardiovascular Assessment
The evaluation consisted of the parameters heart rate (HR), systolic blood pressure (SBP) and diastolic blood pressure (DBP). HR was obtained using the Polar FT01® frequency meter, with three components (reader, elastic strap and watch), keeping the participants in the orthostatic position during the exam. SBP and DBP were measured with an aneroid sphygmomanometer (Premium®), previously calibrated by the National Institute of Metrology, Quality and Technology (InMetro) and stethoscope (Premium Rappaport®), using a technique standardized by the 7th Brazilian Directive on Arterial Hypertension [14].
Glycemic Control
The analysis of glycemic control took place through capillary blood glucose, where the Accu-Check® device was used. The reason for using this method was due to its low cost and easy access; availability of equipment and supplies at the study site; obtaining immediate results; and as a motivating factor for the adherence of participants to the study, as it allows the practical assessment of the effects of interventions, especially physical exercises.
Muscle Strength Assessment
It consisted of tests of 1RM in the bench press and leg press machines [15].
Study Interventions
In the education program, illustrative posters prepared by the researchers were used, relating to the general management of the disease, to self-care, which included the following themes: description of the disease process and treatment modalities; practice of physical activity integrated into the lifestyle; blood glucose monitoring and its interpretation; body weight control; proper use of medications; and prevention of complications. In the physical training program, the concurrent training methodology was adopted (aerobic physical exercises in combination with anaerobic or resistance physical exercises) with three weekly sessions, one hour long, and moderate to intense intensity.
The physical training methodology adopted was concurrent training, characterized by aerobic physical exercises in combination with resistance physical exercises. The training sessions took place at CESEF, 3 weekly sessions lasting 60 minutes. Aerobic exercise occurred on elliptical, treadmill and bicycle ergometers with moderate intensity and duration of 3 minutes. Resistance training was performed on weight machines, with 3 sets, 12 repetitions, with a 1-minute interval between sets and exercises, moderate intensity (50% of 1RM), 30 minutes of duration and where the main muscle groups of the upper and lower limbs [16].
Statistical Analysis
The collected data were double-entered in the MS-Excel application and then processed electronically for validation. Subsequently, the data sheet was exported to the GraphPad InStat software, version 3.10 (public domain). Numerical data related to anthropometric, cardiovascular, muscle strength and glycemic parameters were submitted to the Komolgorow-Smirnov and Levene tests to verify, respectively, the normal distribution and homogeneity of variances.
For comparisons between two dependent samples (between the follow-up assessments, as well as in the comparison of these with the detraining one), the paired t-test was used, since the normal distribution was evidenced. The results were expressed as mean and standard deviation, with a significance level (p) lower than 0.05.
Results
In the present study, no significant reductions were found in the anthropometric parameters studied (body weight, BMI, and waist circumference), shown in Figure 02. A continuous reduction in all values compared to the 1st evaluation (beginning of the study) is observed, making to increase after the pandemic period, represented by the 5th assessment (end of the study). The mean (±SD) of body weight in the first assessment was 78.6±15.8 kg and reduced to 72.4±14.1 kg in the fourth assessment but increased to 76.0±15.1 kg later. of the pandemic. The same behavior was observed in BMI, whose average in the first evaluation was 32.5±6.5 kg/m2 (grade 1 obesity), reduced to 28.6±5.2 kg/m2 (overweight) in the fourth evaluation and increased to 31.5±6.2 kg/m2 (grade 1 obesity). The mean waist circumference in the first evaluation was 109.5 ±12.7 cm, reduced to 103.6 ±9.6 cm in the fourth evaluation and returned to 109.7±11.9 cm. However, the waist circumference results throughout the study showed values above normal.
Figure 2: Behavior of anthropometric parameters.

(Figure 3) presents the average results of the HR behavior in all evaluations, being before the performance and post at the end of it.
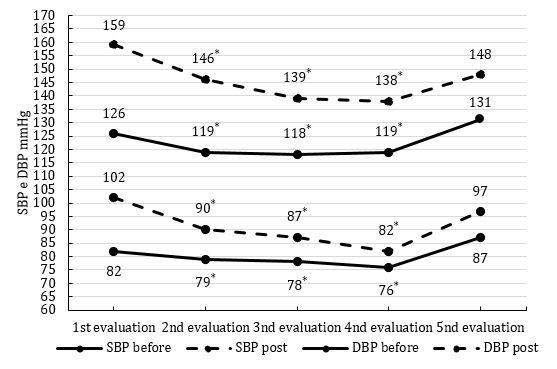
It is observed that the behavior of the heart rate results is like those found in the anthropometric parameters, continuous reduction throughout the first four assessments with an increase after the pandemic, represented in the fifth assessment. The values in the second, third and fourth evaluations are significantly lower when compared to the result in the fifth evaluation, both in pre and post values. The mean values of SBP and DBP before and after the five assessments are shown in Figure 4. They were significantly reduced between the 2nd, 3rd and 4th assessments when compared to the 5th assessment.
Figure 3: Behavior of HR parameter.
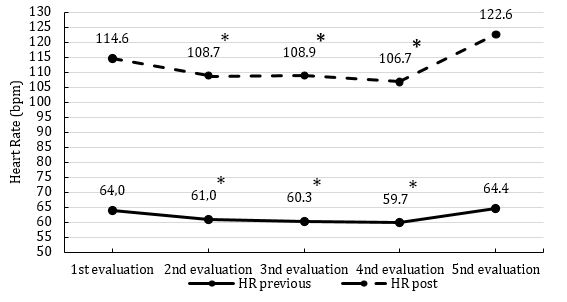
Figure 4: Behavior of SBP and DBP parameters.
This behavior of blood glucose, both in pre and post evaluation are shown in figure 5, also in average values for pre (previous) and post (post) to each evaluation.
Figure 5: Behavior of Blood Glucose parameter.
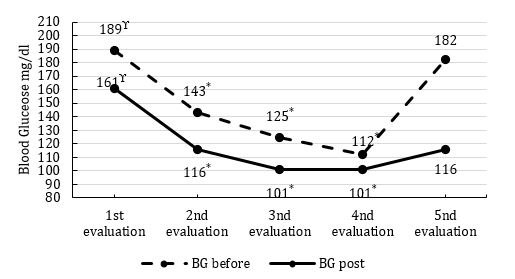
* Significant difference between 2nd, 3rd, and 4th assessments with the 5th assessment.
ϒSignificant difference between 2nd, 3rd, and 4th assessments with the 1st assessment. P < 0.05
Regarding the mean values of muscle strength, analyzed by the 1RM tests in the bench press and leg press machines, no significant differences were found in leg press for both pre and post evaluation mean values. However, for the 1RM test in the bench press, significant differences were observed between the 2nd, 3rd and 4th evaluations when compared to the 1st evaluation. But from these evaluations for the 5th evaluation carried out after the pandemic, there was an increase, but without significance (Figure 6).
Figure 6: Behavior of Muscle Strength parameter.
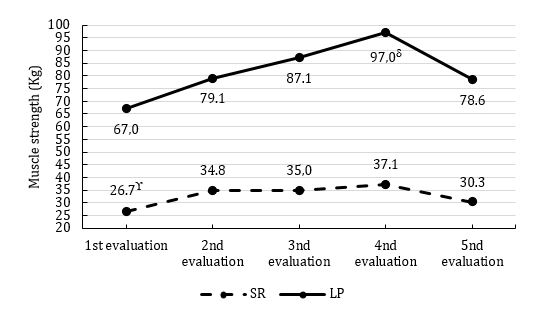
ϒ Significant difference between 2nd, 3rd, and 4th assessments with the 1st assessment.
δ Significant difference between the 4th assessment and the 1st assessment. P < 0.05
Discussion
The aim of the study was to perform anthropometric, cardiovascular, glycemic control and muscle strength assessments in diabetic volunteers after the interruption of the program, and to compare the results with those obtained prior to the Covid-19 pandemic. The hypothesis was that the parameters studied, during the concurrent training program, would show improvements that would be reversed during the Covid-19 pandemic period due to the effect of detraining.
Anthropometric Parameters
Regarding the anthropometric parameters studied (body weight, waist circumference and BMI), continuous reductions in values were observed, but without statistical significance during the concurrent training period. When compared to post-pandemic values, there were increases in the results, but also without significance.
Body weight and BMI parameters were studied in 47 volunteers (mean age 70 years) who participated in a training period of 9 consecutive months, with 86 sessions of 45 minutes duration, consisting of cardiorespiratory and resistance exercises of moderate intensity. After the training period, the volunteers were instructed to maintain their normal lifestyles that included eating patterns and physical routines, but without participating in a systematic exercise program for three months (detraining period), in which significant changes were observed. When comparing with the results of the present study, the same behavior of body weight and BMI was noticed, a reduction during the training period, but after the interruption, the values returned to the pre-training results, however, without statistical significance [17].
The difference in the results of the parameters analyzed between the studies can perhaps be explained by the training and untraining time, as well as by the size and characteristics of the studied samples. In the present study, there were two years of training and detraining, while in the study, there were 9 months of training with 3 months of detraining. This 21-month difference in detraining is quite significant for reducing training-induced physiological adaptations, even if it was for 2 years. The interruption of training or its marked reduction, present in the pandemic period, can almost completely reverse the induced physiological adaptations, which is called the principle of reversibility [18]. Another important detail is that, in the study, it was suggested that the volunteers maintain their patterns of physical routines, which were possibly not drastically interrupted because they were not in a pandemic scenario, contrary to what happened in the present investigation. The presence of non-communicable chronic diseases, as characterized in the investigated sample, was also not made explicit in the study. This difference is important for the ability to train and, added to the other circumstances mentioned, are factors that could contribute to the lack of statistical significance between the times of the parameters studied.
Another study analyzed the behavior of BMI, after detraining, in 37 diabetic volunteers, aged between 69 and 72 years, who participated in a circuit training program composed of aerobic exercises, muscle strengthening and stretching. Three weekly sessions of one hour duration and moderate to high intensity were performed for 12 weeks, followed by eight weeks of detraining. The results showed no significant differences in pre-training, post-training and post-detraining BMI values [19]. This behavior differs from that of the present study, in which there was a continuous reduction in values as the training lengthened. After the pandemic, the values returned to those observed in the 1st evaluation, which corresponded to the beginning of the training program, without statistical significance. It can be inferred that this difference in the BMI results found between the studies may be due to the training and detraining time. The methodology in this last study was just 12 weeks of training with 8 weeks of detraining, which is shorter than those proposed in the present research. Such difference could have contributed for the results of the present study to be, even if not significant, more satisfactory for the control of glycemia in diabetic patients.
The effect of detraining on body weight and BMI was also studied in diabetic volunteers who performed different models of physical training. Thirty volunteers aged 48.1±1.7 years, body weight of 71.7±6.1 Kg, BMI of 26.0±2.1 Kg/m2, on average, participated in a physical training program lasting 12 weeks (either aerobic training or resistance training) and 6 weeks of detraining. The results showed a reduction in body weight and BMI values during training in both groups, but in the aerobic group, both parameters remained close to the values at the end of training. This indicates that aerobic training is more efficient in promoting more significant physiological adaptations than resistance training. In the present study, the values of both parameters at the end of the pandemic (5th assessment) were lower than those obtained in the 1st assessment. The difference in these results between the samples can be explained by the training time and the training model proposed in the present study. In the study mentioned above, the group participated in a training program either aerobic or resistance for 12 weeks and, in the present investigation, concurrent training was prescribed (aerobic and resistance in the same session), lasting 24 months, followed by detraining in same period. The longer training time could have provided significant adaptations, which would require more detraining time to return to baseline values [20].
Cardiovascular Parameters
The behavior of cardiovascular parameters (HR, SBP and DBP) in the present study was similar, that is, the values reduced during the concurrent training program (2nd, 3rd, and 4th evaluations) and significantly increased to those of pre-training, after the detraining occurred in the COVID-19 pandemic (5th assessment). HR, like all other parameters, was assessed before and after each session. Regarding their pre and post behavior, significant reductions were observed during the concurrent training period (2nd, 3rd, and 4th evaluations) in relation to the result of the 5th evaluation. These findings are corroborated by a study that analyzed the behavior of cardiovascular parameters in 47 elderly women who underwent training for 9 months, with cardiorespiratory and resistance exercises of moderate intensity, and then remained in three months of detraining. The results showed significant increases in the behavior of HR, SBP and DBP after the detraining period. The authors concluded that the respective period was sufficient to promote hemodynamic decline in elderly women and suggest that it should be avoided [17]. However, in the present study, the detraining period was very long (two years) compared to the study, which coincided with the period of the pandemic. The increase in the mean values of HR after detraining can be explained by the increase in sympathetic-adrenergic tone to the myocardium during detraining, and this behavior is directly related to the inactivity time [21]. Diabetic patients, such as the volunteers in the present study, may have cardiac autonomic neuropathy, which is characterized by hyperactivity of the sympathetic autonomic nervous system and consequent progressive loss of parasympathetic cardiac inflow, thus losing cardioprotective function [22]. This change in the autonomic adjustments in the heart, with an increase in sympathetic tone and consequently cardioaccelerator, could explain this significant increase in HR behavior both at rest (pre) and at the end of the concurrent training session (post), after the pandemic.
Regarding the other cardiovascular parameters, SBP and DBP, shown in figure 4, the same behavior of HR is observed. A significant reduction during the concurrent training program and, after the pandemic, uplift to both PAS and PAD. The explanation for this behavior in SBP may be related to the adaptations induced by concurrent training, which is characterized by being composed of aerobic exercises combined with resistance exercises. In this case, the training program induced specific adaptations, both anatomical and physiological, which are imposed by the pressure and volume loads of physical exercises. During aerobic exercise, there is a persistent increase in cardiac output, which stimulates left ventricular chamber dilation. In resistance exercises, due to the elevation of intrathoracic pressure, there are compensatory increases in the thickness of the left ventricle [24]. These cardiac anatomical adaptations make the heart more efficient, reducing HR at rest and at the same exertion load and, as a result, reducing SBP [24].
The DBP is related to the peripheral resistance that regulates the blood supply to the tissues, due to its flow through the conductance vessels, so the pressure will rise with an increase in the systemic resistance [25]. Elevation in peripheral resistance may occur due to loss of arterial elasticity due to gradual fragmentation and loss of elastic fibers and accumulation of collagen fibers [26].
However, the process of arterial stiffening may be accelerated with aging and mainly by DM [27]. In the present study, significant reductions in DBP are observed both pre- and post-assessment. These results are corroborated by a study that analyzed arterial stiffening in 36 diabetics (71.4±0.7 years), who performed physical training for three months, in three weekly sessions lasting 60 minutes each, with an aerobic group (treadmill treadmill and cycle ergometer) and non-aerobic (exercise with ball and dumbbells). The results demonstrate the effectiveness of aerobic training in reducing arterial stiffening [27].
However, when studying the effect of a predominantly anaerobic exercise model, the results corroborate those observed in the present investigation. In the study by Andrade et al. (2022), SBP, DBP, HR and postprandial blood glucose were evaluated in 22 diabetic volunteers who were divided into a control group and a Pilates group. The authors observed significant reductions in the 4th and 8th weeks of training in DBP [28], results that are similar to those of the present study.
The interruption of training or detraining induces serious adjustments to the cardiovascular system, including cardiac atrophy observed in short periods, between the 1st and 8th week. This cardiac atrophy may be closely associated with reductions in anatomical and physiological adaptations (ventricular mass and thickness) induced by the training program, which may compromise physical performance characterized by significant increases in the parameters studied, HR, SBP and DBP [23].
Glycemic Control
Among all the parameters studied, the behavior of blood glucose was the one that most changed during the study. In the 1st evaluation (beginning of the study) the mean value at rest, immediately before the performance of the first training session, was 189mg/dl, however it reduced significantly in the 2nd, 3rd, and 4th evaluations (respectively, 143mg/dl, 125mg/dl and 112mg/dl or -25%, -34% and -41%). However, in the 5th evaluation (post-pandemic detraining period) the mean value rose significantly to 182mg/dl or 62.5% of the result obtained in the 4th evaluation.
The same behaviour was presented in the analyzes that occurred at the end of each evaluation or at the moment after. The mean value was 161mg/dl and significantly reduced in the 2nd, 3rd, and 4th evaluations (respectively 116mg/dl, 101mg/dl and 101mg/dl or -28%, -37% and -37%). As observed in the pre-session, the mean blood glucose value in the 5th assessment was 116mg/dl or 12%.
This glycemic behavior is corroborated by results obtained in a study with albino-wistar rats, which induced DM by infusion of streptozotocin, and the animals were divided into a control group and an aerobic training group (three sessions per week for eight weeks, followed by four weeks of detraining). The authors observed a significant reduction in blood glucose, glycated hemoglobin, and insulin during the eight-week period of training, but these values significantly increased again after the four weeks of detraining [29]. When compared with the results obtained in the present study, there are differences in the sample and methodology of the training program and despite this, the results are similar. A study in elderly women showed the same behavior of blood glucose at rest. A total of 28 volunteers, with a mean age of 70.3±2.3 years, participated in a multicomponent training program (a program that exercised all physical skills: endurance, muscular strength, coordination, flexibility, and balance) for nine months, being 86 training sessions, lasting 45 minutes, two weekly sessions and at the end, detraining for 3 months. The results showed a significant increase in glycemic values at rest after the detraining period when compared to the values at the end of the multicomponent training period [17].
The training methodology was also studied in relation to the behavior of glycemia and glycated hemoglobin in another research. In this, 30 volunteers of both sexes, 48.1±1.7 years old, 71.7±6.1Kg and 26.0±2.1 Kg/m2, were divided into an aerobic group and a resistance group, the training program was six weeks followed by the same period of detraining. The results showed a significant reduction in mean blood glucose values at the end of the training period, however, a significant increase in the same results at the end of the detraining period [20]. There are differences in the training methodology between the study and the present study, in which there were two years of training, but also two years of detraining caused by the pandemic. Despite being different times, the proportionality between training and detraining period were similar in both studies and demonstrates the importance of physical exercise in glycemic control.
Participation in a physical training program (aerobic, resistance and concurrent) induces important adaptations in adipocytes and skeletal muscles that will allow type 2 diabetics to control their blood glucose [30]. In adipocytes, exercise mainly improves insulin signaling steps [31]; modulates the expression and release of adipokines [32, 33] and reduces the size of adipose tissue, mainly visceral [34].
Insulin acts on numerous tissues, but mainly on the liver, adipose tissue, and skeletal muscles by promoting, mainly, the elevation of glucose uptake through a process called the insulin cascade. Physical training induces an increase in the protein expression of glucose transporters (Glut4), in the activation of molecules present in the insulin cascade, such as insulin receptor substrates 1 (IRS-1), phosphoinositide 3 kinase (PI3K) and protein kinase B (Akt) and, therefore, increased glucose uptake by tissues [31].
In obese individuals, adipose tissue behaves like an inflamed tissue, increases the expression of pro-inflammatory adipokines (TNF-alpha, IL1-beta, IL-6, among others) and inhibits anti-inflammatory (adiponectin). This effect increases insulin resistance in skeletal muscles and adipose tissue, by activating the phosphorylation of the serine/tyrosine pathway that acts in the inhibition, mainly of IRS-1 [31]. Participation in a six-week aerobic training program was sufficient to significantly reduce TNF-alpha values and improve glycemic control in diabetics [32].
The reduction in the size of adipose tissue, mainly visceral, is an important physiological adaptation induced by physical training in diabetics. By reducing its size, mainly visceral, it reduces the expression and release of pro-inflammatory adipokines and elevates the anti-inflammatory, which reduces insulin resistance [33].
In skeletal muscles, participation in a training program increases glucose uptake, expression, and translocation of Glut4 mainly, which will allow glycemic control in diabetics [30]. Skeletal muscle is one of the most dynamic and plastic tissues in the human body, representing approximately 40% of total body mass or about 50% to 75% of all body proteins. It is a metabolically active tissue, mainly during physical exercise [34]. In addition to these characteristics, skeletal muscle also plays an important role in the control of postprandial blood glucose, about 80% of all ingested glucose is absorbed through insulin-dependent uptake [35]. Insulin is one of the main glycemic control hormones and the membrane of the skeletal muscle fiber has receptors that, when stimulated, activate the IR/IRS/PI3K/Akt pathway that promotes the translocation of glucose transporters (Glut4) and the uptake of glucose [36].
However, insulin is not the only mechanism for glucose uptake by skeletal muscles [37]. Physical exercise also increases your glucose uptake capacity through muscle contraction. In models of acute physical training, muscle contractions induce an increase in energy demand by increasing glycolysis and oxidative phosphorylation of adenosine triphosphate (ATP) [38]. Elevation of ATP oxidative phosphorylation reduces its AMP/ATP ratio and, consequently, the activation of adenosine monophosphate-activated protein kinase (AMPK). Activation of AMPK increases glucose uptake in skeletal muscles, active by increasing the translocation and expression of the glucose transporter (Glut4) from the cytoplasm to the cell membrane of the muscle fiber [39, 40].
Muscle contraction also activates another glucose uptake pathway by increasing intracellular calcium concentration. This pathway is called calcium/calmodulin signaling dependent on protein kinase (CMPK) and, when activated, promotes the translocation of Glut4 [40]. In chronic models, physical exercise increases glucose uptake by muscles by increasing insulin sensitivity [41]. Effectively, diabetic volunteers have the same glucose uptake capabilities as non-diabetics [40].
The interruption in the partial or even total training program induces different anatomical and physiological changes both in the short and in the long term [18, 21]. Among the consequences of detraining, there is dysregulation of insulin secretion and blood glucose concentration, and a decrease in the glucose transporter, GLUT4 [20]. In the present study, the adaptations described in adipocytes or even in skeletal muscles were not analyzed, however, we observed significant reductions in glycemia in pre and post evaluation during the period of concurrent physical training, which were reversed by the detraining induced by the pandemic.
Muscle Strength Parameter
Figure 6 shows the mean values of the tests performed by diabetic volunteers to measure muscle strength. Regarding the bench press exercise, significant elevations were found in the 2nd, 3rd, and 4th evaluations in relation to the 1st evaluation, which represents the beginning of the training program. But no differences were found between the assessments before and after the pandemic. Regarding the leg press exercise, a significant difference was found only in the 4th assessment in relation to the 1st assessment.
In one study, 18 women aged 55.8±5.1 years and 9.8±5.4 years diagnosed with DM, on average, participated in a concurrent training program for nine months and achieved significant improvements in muscle strength. However, they interrupted training for three months (detraining), and muscle strength values reduced, but remained significantly higher than resting values [42]. This behavior in muscle strength was also observed in the present study, in which muscle strength increased during the training program and decreased during the detraining period, but with higher values than those observed in the 1st evaluation.
With aging, there is a progressive reduction in skeletal muscle mass and strength, called sarcopenia [43]. This loss occurs more markedly in diabetic patients compared to age-matched normoglycemic patients and denotes that it is age-related and is accelerated by the loss of glycemic control [44]. Studies suggest that this sarcopenia is due to the atrophy of type 2 skeletal muscle fibers [43] which have anaerobic metabolic characteristics, high production of force and tension [44].
Final Considerations
Participation in a session or in a physical training program with a predominance of aerobic or resistance exercises or their combination revealed to be important non-pharmacological tools for glycemic control. In the present investigation, a 24-month program of concurrent training promoted important physiological adaptations observed in anthropometric, cardiovascular, glycemic control and muscle strength in type 2 diabetic volunteers. However, its complete interruption, characterized by detraining (principle of reversibility in training), longer than 4 weeks, interrupted the improvements in physical performance and induced a complete reversal of the adaptations in the parameters studied, with impairment of physical fitness, glycemic control, and cardiovascular performance. The concurrent training program, of this duration, was not enough to prevent the physiological losses imposed by detraining, thus denoting the importance of continuous and uninterrupted participation in this training model for type 2 diabetic individuals.
Acknowledgments
We thank Fernando Inocêncio de Brito, Alinson Eduardo Cipriano and Ana Paula de Gouveia for their help in data collection.
References
- Sociedade Brasileira de Diabetes (2019) Diretrizes da Sociedade Brasileira de Diabetes 2019-2020. São Paulo: Clannad 491 P.
- International Diabetes Federation (2019) IDF Diabetes Atlas. 9th ed. 176 p.
- Muzy J, Campos MR, Emmerick I, Sabino R (2022) Oferta e demanda de procedimentos atribuíveis ao diabetes mellitus e suas complicações no Brasil. Ciência & Saúde Coletiva 27:1653-1667.
- Oliveira PSD, Dias JLC, Nunes RLN, Oliveria PA, Magalhães PGA, et al. (2022) Complicações do diabetes no estado de Minas Gerais no período de 2012 a 2013. Rev Enferm Atual in Derme 96: e-021245.
- Bao Y, Sun Y, Meng S, Shi J, Lu L (2020) 2019-nCoV epidemic: address mental health care to empower society. Lancet 395: e37-e38.
- Lake MA (2020) What we know so far: COVID-19 current clinical knowledge and research. Clin Med (Lond) 20: 124-127.
- Liu YC, Kuo RL, Shih SR (2020) COVID-19: The first documented coronavirus pandemic in history. Biomedical Journal 43.
- Croda J, Oliveira WK, Frutuoso RL, Mandetta LH, Baia-da-Silva DC, et al. (2020) COVID-19 in Brazil: advantages of a socialized unified health system and preparation to contain cases. Rev Soc Bras Med Trop 53: e20200167.
- Neiva MB, Carvalho I, Costa Filho ES, Barbosa-Junior F, Bernardi FA, et al.(2020) Brazil: the emerging epicenter of COVID-19 pandemic. Rev Soc Bras Med Trop 53: e20200550.
- Rosa MFP, Silva WNT, Carvalho WRG, Oliveira SV (2020) Epidemiologia da COVID-19 em Uberlândia (MG): análise preliminar do impacto do grau de abertura comercial. J Health NPEPS 5: 20-41.
- Polit DF, Beck CT. (2011) Fundamentos de pesquisa em enfermagem: avaliação de evidências para a prática da enfermagem. 7 ed. Artmed, Porto Alegre, Brasil.
- Moraes NM, Souza GFP, Brito FI, Antonio Júnior ME, Cipriano AE, et al. (2020) Knowledge about diabetes mellitus and self-care activities before and after an educational program: a pilot study. OJN10:101-116.
- Gomes LC, Moraes NM, Souza GFP, Brito FI, Antônio Júnior ME, et al. (2021) Contribuições de um programa educativo na prevenção de lesões nos pés de pessoas com diabetes mellitus. J Health NPEPS 6: 62-86.
- Malachias MVB, Souza WKSB, Plavnik FL, Rodrigues CIS, Brandão AA, et al. (2016) 7ª Diretriz Brasileira de Hipertensão Arterial. Arq. bras. cardiol 107:1-83.
- Delavier, F (2012) Guia dos movimentos de musculação: abordagem anatômica. São Paulo: Editora Manole, 192 p.
- Colberg S, Parson HKP, Nunnold T, Holton D, Vinik AI (2010) Exercise and type 2 diabetes. Diabetes Care 33.
- Leitão L, Pereira A, Mazini M, Venturini G, Campos Y, et al. (2019) Effects of three months of detraining on the health profile of older women after a multicomponent exercise program. Int. J. Environ. Res. Public Health 16: 3881.
- Mujika I, Padilla S. Detraining: loss of training-induced physiological and performance adaptations. part I - short term insufficient training stimulus. Sports Med 2000a Aug 30: 79-87.
- Park SY, Lee IH (2014) Effects on training and detraining on physical function, control of diabetes and anthropometrics in type 2 diabetes; a randomized controlled trial. Physiother Theory Pract 1–6
- Farias TY, Santos-Lozano A, Urra PS, Cristi-Montero C (2015) Effects of training and detraining on glycosylated haemoglobin, glycaemia, and lipid profile in type-II diabetics. Nutr Hosp 32: 1729-1734.
- Mujika I, Padilla S. Detraining: loss of training-induced physiological and performance adaptations. part II - long term insufficient training stimulus. Sports Med 2000b Sep 30: 145-154.
- Voulgari C, Pagoni S, Vinik A, Poirier P. (2013) Exercise improves cardiac autonomic function in obesity and diabetes. Metabolism Clinical and Experimental 62: 609–621.
- Petek BJ, Groezinger EY, Pedlar CR, Baggish AL (2022) Cardiac effects of detraining in athletes: A narrative review. Annals of Physical and Rehabilitation Medicine 65: 101581.
- Alom AA, Bhuiyan NI, Horrain NM, Hoque MF, Rozario RJ, et al. (2011). Physical training induced resting bradycardia and its association with cardiac autonomic nervous activities. Mymensingh Medical Journal: MMJ 20: 665-670.
- Simone G, Pasanisi F (2001) Systolic, diastolic and pulse pressure: pathophusiology. Ital Heart J Supl 2: 359-362.
- Oh YS (2018) Arterial stiffness and hypertension. Clinical Hypertension 24:17
- Madden KM, Lockhart C, Cuff D, Potter TF, Meneilly GS (2009) Short-term aerobic exercise reduces arterial stiffness in older adults with type 2 diabetes, hypertension, and hypercholesterolemia. Diabetes Care 32:1531–1535.
- Andrade IYTP, Melo KCB, Andre KTP, Almeida LG, Moreira SR (2022) Pilates training reduces blood pressure in older women with type 2 diabetes: A randomized controlled trial. Journal of Bodywork & Movement Therapies 30:168e175.
- Omidi M, Yousefi M (2019) The effect of 1 week of aerobic exercise and 4 weeks of non-exercise on fasting glucose, insulin and blood serum glycosylated hemoglobin concentration of diabetic rats treated with streptozotocin. Journal of Practical Studies at Bioscience in Sport 7: 55-64.
- Andrade EF, Oliveira Silva V, Orlando DR, Pereira LJ (2019) Mechanisms Involved in Glycemic Control Promoted by Exercise in Diabetics. Current Diabetes Reviews 15: 105-110.
- Mann G, Ridell MC, Adegoke OAJ (2022) Effects of Acute Muscle Contraction on the Key Molecules in Insulin and Akt Signaling in Skeletal Muscle in Health and in Insulin Resistant States. Diabetology 3: 423–446.
- Molnár A, Szentpéreri A, Lörincz H, Seres I, Harangi M, et al. (2022) Change of Fibroblast Growth Factor 21 Level Correlates with the Severity of Diabetic Sensory Polyneuropathy after Six-Week Physical Activity. Rev. Cardiovasc. Med 23: 160.
- Lee-Ødegård S, Olsen T, Norheim F, Drevon CA, Birkeland KI, et al. (2022) Potential Mechanisms for How Long-Term Physical Activity May Reduce Insulin Resistance. Metabolites 12: 208.
- Frontera WR, Ochala J (2015) Skeletal Muscle: A Brief Review of Structure and Function. Calcified Tissue International 96: 183–195.
- Böhm A, Weight C, Staiger H, Häring H (2016) Exercise, and diabetes: relevance and causes for response variability. Endocrine 51: 390–401.
- Karlsson HKR, Zierath JR (2007) Insulin signaling and glucose transport in insulin resistant human skeletal muscle. Cell Biochem Biophys 48: 103–113.
- Hulett NA, Scalzo RL, Reusch JEB (2022) Glucose Uptake by Skeletal Muscle within the Contexts of Type 2 Diabetes and Exercise: An Integrated Approach. Nutrients 14: 647.
- Stanford KI, Goodyear LJ (2014) Exercise and type 2 diabetes: Molecular mechanisms regulating glucose uptake in skeletal muscle. Adv. Physiol. Educ. 38: 308–314.
- Bonab SB, Dastah S Performing training in water improves glucose homeostasis and lipocalins in women with type 2 diabetes mellitus. Sci sports.
- Yaribeygi H, Atkin SL, Simental-Mendia LE, Sahebkar A (2019) Molecular mechanisms by which aerobic exercise induces insulin sensitivity. J. Cell Physiol 234: 12385–12392.
- Tokmakidis SP, Touvra A-M, Douda HT, Smilios I, Kotsa K, et al. (2014) Training, Detraining, and Retraining Effects on Glycemic Control and Physical Fitness in Women with Type 2 Diabetes. Horm Metab Res 46: 974–979.
- Leenders M, Verdijk LB, Hoeven LV, Adam, JJ, Krnenburg, JV, et al. (2013) Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. JAMDA 14 585e592.
- Park SW, Goodpaster BH, Strotmeyer ES, Kuller, LH, Broudeau R, et al. (2007) Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: The health, aging, and body composition study. Diabetes Care 30:1507e1512.
- Zumbauch MD, Johnson SE, Shi TH, Gerrard DE (2022) Molecular and biochemical regulation of skeletal muscle metabolism. Journal of Animal Science100: skac035.