Melanocyte Growth Factor Deprivation is Intertwined with Oxidative Stress and Autoimmune Theories in the Etiology of Vitiligo. A Basis for Treating Vitiligo.
Ramaiah Abburi1*
1 Samastha Laboratories Hyderabad, India.
*Corresponding Author: Ramaiah Abburi, Samastha Laboratories Hyderabad, India, Tel: +098490 66543; Fax: 00-+098490 66543; E-mail:ramaiah_abburi@yahoo.com
Citation: Ramaiah Abburi (2023) Melanocyte Growth Factor Deprivation is Intertwined with Oxidative Stress and Autoimmune Theories in the Etiology of Vitiligo. A Basis for Treating Vitiligo. Medcina Intern 5: 172
Received: February 15, 2023; Accepted: February 24, 2023; Published: February 28, 2023.
Copyright: © 2023 Ramaiah Abburi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
In the present communication, I will discuss how melanocyte growth factor deprivation theory as cause of vitiligo is intertwined with the other prevailing theories of oxidative stress and auto immunity. Based on the growth factor deprivation theory as one of possible causes for loss of melanocytes in vitiligo, experiments were done to develop a therapeutic agent to treat vitligo. The active basic fibroblast growth factor related peptides (bFGFRP) act as mitogen on melanocytes in culture or in mixed cultures of melanocytes and keratinocytes obtained from untreated vitiligo patients. bFGFRP increases repigmentation of depigmented patches in experimental animal models compared to corresponding controls. bFGFRP was considered as potential repigmenting agent for vitiligo macules. Various phases of clinical trials were conducted in India to study the safety and efficacy of the bFGFRP in patients with vitiligo. Based on the results of these trials, the deca peptide (bFGFRP) was listed as a drug to treat vitiligo in 2001 and sold in India by trade names Melgain and Melbild and other names.
The protocols on using bFGFRP to treat vitiligo will be described in detail not only as a single agent for non-segmental and segmental vitiligo but also in combination with PUVA/PUVASOL, vitiligo resistant to further treatment with PUVA, NBUVB or with steroids or with surgical procedures.
Introduction
Vitiligo is an acquired depigmentary disorder characterized by the patchy depigmentation of skin that may become progressive over time. It affects both sexes. Barring the loss of pigment, the depigmented patches are otherwise normal in all other respects.
Causes of the Disease
The etiology of the disease is far from clear (1). Recent experimental and clinical related evidence suggests that the vitiligo melanocytes are more prone to oxidative stress than the normal melanocytes (2). The sensitivity of melanocytes to oxidative stress is interlinked with melanocyte growth factor deprivation theory as proposed by us (3) and of autoimmunity (4-5). It is generally believed that the vitiligo skin is devoid of pigment producing cells – melanocytes. But recent studies however confirm the lone earlier observation (6) that the vitiligo skin does contain non-functional melanocytes and that they could be made functional to produce pigment under certain conditions invitro (7).
Implications of the Disease
The patchy depigmentation of skin is disfiguring and thus often produces psychological trauma which could lead to depression or social withdrawal of the vitiligo affected individual. The chances of sunburn of the skin increase because of this depigmentation.
World Scenario
Vitiligo affects about 1% of the world population without racial, sexual or regional differences. But some reports suggest that the incidence in India, Egypt and Japan is higher, and it ranges from 1.25% to 6% of the population (8).
Present Major Methods of treatment of the Disease
The major method of treatment of the disease worldwide is by photo chemotherapy using psoralens followed by ultraviolet A radiation, which is based on the observations described in Atharva Veda, more than 3000 years ago. But such treatment has many undesirable side effects, and its success rate is on an average about 50% and that too, often the patches rarely repigment completely. Similarly, the other methods available to treat vitiligo (9) are not completely effective and have some undesirable side effects.
The New Approach to treat vitiligo: The new approach to treat vitiligo was based on our hypothesis published earlier (3, 11, and 13). We hypothesized that vitiligo could be treated by growth factors to maintain and proliferate the melanocytes. It was observed that the melanocytes from untreated vitiligo subjects, when grown in culture had abnormal growth characteristics compared to the melanocytes from normal subjects and the perilesional melanocytes exhibit abnormal morphology (11). The abnormal growth characteristics of melanocytes and the abnormal morphology of perlesional melanocytes are summarized in Table 1 and shown In Figure
Figure 1: The Melanocytes from Normal, the perilesional &far away from the vitiligo macule.

Melanocytes (N) Melanocytes V(Far away) Melanocytes(Perilesional) Taken from (11)
Table1: Growth Characteristics of Normal and Vitiligo Melanocytes.
Taken from (3, 11) These abnormal growth characteristics were partially corrected by the addition of 100,000g supernatant of the homogenates of fibroblasts grown invitro to the growth medium of melanocytes from the untreated vitiligo subjects (12). These abnormal growth characteristics disappeared completely in melanocytes obtained from the successfully treated vitiligo lesional, and perilesional areas of successfully treated vitiligo subject with PUV-A (Psoralenss and UV-A (13). These studies and the fact that addition of serum from the successfully treated vitiligo patients to the culture medium of the melanocytes from the untreated vitiligo patients corrected their abnormal growth, led to our hypothesis that these defects in melanocytes were related to the disease and therefore vitiligo could be treated by growth factors to maintain and proliferate the melanocytes (13). These studies were done by growing melanocytes in a culture medium devoid of any growth factors except forbol ester and cholera toxin (3,11). The other studies done later by others (14) did not observe these defects since their culture conditions were different and always grew the cells in presence of various growth factors. Studies on invitro cell cultures of melanocytes were then conducted to test whether indeed the defective growth characteristics of melanocytes from the perilesional and distant from the lesional area could be corrected by the addition of basic fibroblast growth factor (bFGF). It was observed that addition of bFGF into the culture medium abolished the differences in the growth characteristics of cells from the vitiligo subjects. In addition, bFGF could increase the proliferation of melanocytes and their passagebility obtained from the perilesional areas of untreated vitiligo subjects. In view of the fact that melanocytes constitute a small proportion of cell of the epidermis and that keratinocytes constitute more than 95% of epidermal cells it was necessary to test whether indeed the proliferative effect of bFGF on melanocytes could be demonstrated even in mixed cell cultures of melanocytes and keratinocytes obtained from the perilesional areas of untreated vitiligo subjects. The results indeed demonstrated that bFGF even in mixed cell cultures of melanocytes and keratinocytes stimulated the proliferation of melanocytes as shown in Fig-2.
Figure 2: bFGF increased the proliferation of melanocytes in mixed cultures of keratinocytes and melanocytes from vitiligo patients.

Similar results were obtained with the active fragments of bFGF, (bFGFRP).
Proof of Concept
Thus, bFGF or its active fragments could in principle be used to increase the proliferation of melanocytes in the pigmentation of the vitiligenous area. To demonstrate this in vivo, we developed an animal model of vitiligo.
Development of an animal model for vitiligo: The melanocytes responsible to make melanin in the skin are either non-existent or nonfunctional in vitiligo patches resulting in the white patches on that skin. The guinea pig ear lobes when chemically treated can selectively lose melanocytes resembling vitiligo (15). Similarly, the skin of Yucatan swine, which closely resembles human skin, was chemically treated to lose melanocytes developing vitiligo like skin. Such depigmented white patches were produced on the ear lobes of guinea pigs and shown in Figure 3. The depigmented patches that contain almost no melanocytes on both the ear lobes were used for the study.
Figure 3: Guinea pig ears before and after depigmentation.
Testing the Hypothesis: The growth factor bFGF was interdermally injected into the de-pigmented patches of ear lobes of guinea pigs and the rate of re-pigmentation was compared with corresponding untreated de-pigmented contralateral ear lobes. It was found that interdermally injected bFGF enhanced the rate of re-pigmentation compared to the corresponding contralateral control ear lobe. Similar results were obtained by interdermal injection of the active fragments of bFGF (data not shown). These studies on experimental animals thus provide the proof of the concept. Smaller fragments of active bFGF peptides were preferred because delivery of bFGF by injection in to white patches of vitiligo subjects is not a practical proposition to treat vitiligo. bFGF is 146 amino acid residue long protein with a molecular weight of about 15 K Da. Therefore, smaller bioactive peptides corresponding to various lengths of bFGF were synthesized by solid phase peptide synthesis. These peptides were first interdermally injected to insure their delivery into the epidermis. They were indeed found to increase the rate of repigmentation of depigmented patches of ear lobes of guinea pigs as mentioned above. When the bFGFRP was topically applied in a formulation on the depigmented ear lobes of guinea pig, fast repigmentation resulted compared to the corresponding controls as shown in Figure 4. Similar results were obtained in a number of guinea pigs.
Figure4: Effect of bFGFRP on the repigmentation of depigmented patches of guinea pig ear lobes compared to controls.
Yucatan Swine as more appropriate animal model for vitiligo: The skin of Yucatan swine resembles the human skin and thus studies on Yucatan swine are more appropriate than the guinea pig skin. Therefore, the efficacy of topical application of bFGFRP to repigment depigmented skin of Yucatan swine was studied. Here, again the studies were done on many depigmented patches of Yucatan swine skin. The repigmentation rate of the bFGFRP applied depigmented patches is statistically significant compared to the corresponding placebo treated controls. The effect of various concentrations of decapeptide on the repigmentation of depigmented skin of Yucatan swine presented in figure 5 in a particular formulation indicate that the effect of bFGFRP to repigment is concentration dependent and that it is effective to repigment.
Figure 5: Topical application of (bFGFRP) at varying concentrations on depigmented patches of skin of Yucatan swine.
Development Of Efficient Vehicle to Transport Peptides Through Intact Skin: Interdermal injections are not practical ways of treating vitiligo patients. Therefore, a formulation capable of delivering peptides through intact skin to the epidermis was a necessity. Various vehicles to transport peptide by local application on the intact depigmented skin of experimental animals were tested (data not shown). bFGFRP at various concentrations in various vehicles was tested by local application on the de-pigmented guinea pig ear lobes and on Yucatan swine for their ability to re-pigment the de-pigmented patches. One vehicle was able to deliver the peptide at its lowest concentration, as evidenced by repigmentation of vitiligo macules in the experimental animal model of vitiligo compared to the rest of the vehicles tested (10, 16).
The Animal Model Chosen Here is Appropriate to Test Prospective Drugs to Treat Vitiligo: The animal model used in the experiments described above is appropriate one as shown by the fact PUVA a known method of treatment for vitiligo was shown to repigment faster than the corresponding controls with this animal model (17).
Clinical trials: Preclinical data: The above preclinical data were submitted to the Drug Controller General (India) (DCGI) in 1996 for permission to test the safety and efficacy of bFGFRP on human volunteers. The DCGI gave permission to conduct phase 1 and 2 clinical trials subject to ethical clearances by the institutes concerned. The results of phase 1 and 2 were submitted to the DCGI. The DCGI after being satisfied with the results of phase1 and 2 gave permission for the final phase 3 clinical trials. The total number of volunteers at various phases and of various combinatorial studies is about 300 selected from all over India with variety of ethnic back grounds with 11--V1 type of skin graded according to Fitzpatrick scale.
Phase 1 and 2 Clinical Trials were done at.
- AIIMS Ansari Nagar New Delhi,
- Apollo Hospital Indraprasta, New Delhi,
- Himalayan Institute of Medical Sciences Jolly Grant, Dehraradun,
- St John's Medical College Hospital, Bangalore,
- Owaisi hospital Hyderabad,
- Central Government Unani Hospital Yerra gadda, Hyderabad and at
- Vivekaand Hospital Hyderabad.
Phase 3 Clinical Trials were done at
- Owisi Hospital, Hyderabad,
- St John Medical College Hospital, Bangalore
The clinical trials were conducted for a period of 3-6 months. The vehicle itself had no pigmenting effect on the skin.Early in the clinical trial on human volunteers with bFGFRP, it was observed that exposure of the vitiligo macules to sun 10-15 hours after bFGFRP topical application elicited maximum repigmenting effect. So bFGFRP was routinely topically applied 1-2 hours before going to bed at night and sun exposure of the treated macule the next day morning.
Figure 6: Representative Photographs before & after treatment with bFGFRP.
Figure 7: Representative Photographs before & after treatment with bFGFRP.
Figure 8: Representative Photographs before & after treatment with bFGFRP.
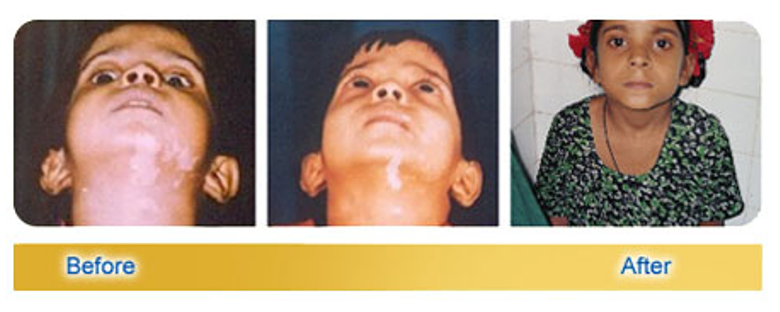
Figure 9: Representative Photographs before & after treatment with bFGFRP.

Combinatorial therapy with bFGFRP +PUVA/PUVASOL: The above vitiligo macules were all localized and small in size. In cases of larger macules, it was felt that an inexpensive PUVASOL in combination with bFGFRP may give faster repigmentation. PUVASOL/PUV-A therapy is perhaps the mainstay in the treatment of vitiligo.However only 50% of cases get repigmentation. Moreover, in a patient in response to PUV-A, many vitiligo macules repigment only partially and the rest of the patches often remain unresponsive to PUV-A therapy even after long duration of treatment (18). More importantly, psoralens have many side effects particularly on the liver and the risk of cancer in the Caucasian skin type II and III population (19, 20). Therefore, there is indeed a need to reduce the
- Duration of the treatment
- To increase success rate
- To treat cases unresponsive to PUV-A therapy.
The above three objectives were accomplished by the combinatorial therapy with bFGFRP+PUVASOL/PUV_A. A Representative picture was shown below (Fig-10). The left hand was the control where psoralens were given orally 2 hours before the sun exposure while the topical application of bFGFRP was applied the night before on the right hand and both were exposed to sun at the same time. It can be seen that there was more repigmentation on the right hand at the end of 3 months of such treatment compared to the control (left hand). These studies were done on 98 volunteers with bFGFRP alone, 18 volunteers with PUV-A alone and 18 volunteers with bFGFRP+PUV-A and the results obtained were found statistically significant.
Figure10: Combinatorial therapy of Vitiligo with bFGFRP + PUV-A SOL.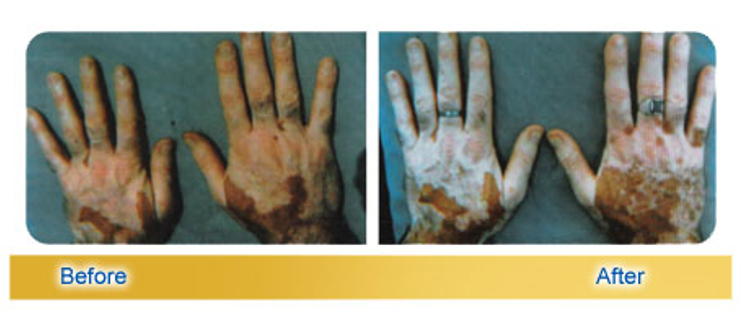
Combinatorial therapy of Vitiligo Resistant to PUV-A with bFGFRP +PUV-A: Whether indeed the macules who did not respond any more to further repigment to PUVA therapy can be made to respond when they were treated in combination with bFGFRP+PUV-A was tested. They indeed responded in all cases with faster repigmentation as in PUVASOl treatment as shown in a representative photograph below (Fig-11, 12).
Figure11: Combinatorial therapy of Vitiligo Resistant to PUV-A with bFGFRP +PUV-A.

Figure12: That this combinatorial therapy was successful even in repigmenting most recalcitrant macules in the palms was shown below.
Synergistic Therapy with Oral Mini Pulse Therapy of Betamethasone and Bfgfrp in Fast Spreading Vitiligo Cases: The clinical trial to treat vitiligo with oral mini pulse (OMP) therapy was first tried by Pasricha et al (21) where they used high oral dose of betamethasone (5mgs) for two consecutive days of the week only called mini pulse therapy. It was felt that a smaller dose of betamethasone could be used if treated with bFGFRP and OMP. Therefore, only 2mgs of betamethasone was given orally on a Saturday and 2 mgs on Sunday of every week during the length of treatment to the volunteers and topical application of bFGFRP as described earlier, with the objective whether this combinatorial therapy was effective to both arrest the fast spread of vitiligo and at the same time results in faster repigmentation than with OMP alone. Betamethasone alone was able to control the spread of the disease even at 2mgs of dose within 6 months and bFGFRP did not play any role in this. But combinatorial therapy of OMP + bFGFRP increased the rate of repigmentation of the macule as shown in a representative figure-13. The ink circled macule was treated with bFGFRP+OMP while the other macules were treated only withOMP. It was done on 16 volunteers with OMP alone and16 volunteers with OMP+bFGFRP and the results were found statistically significant.
Figure 13: Combinatorial therapy of fast spreading Vitiligo with bFGFRP+ OMP
Punch Graft Procedure/or other Surgical Procedures Followed by the Local Application of the Bfgfrp, Synergistic Combinatorial Therapy for the Treatment of Vitiligo Comprising Punch Graft Surgical Procedure: Surgical procedures are the last resort for the treatment of stable vitiligo patches. The procedures include thrish grafting, expansion of autologus melanocytes in culture and their application on to derma-abraded vitiligo patch, autologus expansion of keratinocytes and melaonocytes in culture in the form of a multi cell layered sheets and their application on the derma-abraded vitiligo patches, or punch grafting of pigmented autologus skin on to the derma-abraded vitiligo patches. In the case of punch grafting, after the surgical procedures, the grafted vitiligo patches were surgical bandaged with appropriate antibiotic regimen for the healing of the wounds. The wounds heal within a week. Then the local application of bFGFRP lotion was applied for 3 months. The treated punch grafted patch with bFGFRP showed faster repigmentation uniformly as shown in a representative figure -14. The left hand of 14a was treated with bFGFRP after punch graft while the right hand of 14a only vehicle was applied and exposed to sun similar to left hand after 10-12 hours of the bFGFRP application, while the 14b represents the same after 3 months of the above treatment.
Figure 14: Effect of bFGFRP application after punch Graft.
It was seen that left punch grafted hand treated with bFGFRP repigmented faster than the control (right hand).
Double Blind Randomized Phase IV Clinical Trial on bFGFRP in Vitiligo: All the above-described clinical trials on bFGFRP were open ended. In view of the fact that western countries require only double blind clinical trials on any prospective drug for it to be approved as a drug, a multi-center double blind clinical trial was done on bFGFRP in combination with NBUVB or without. Two macules in non-sun exposed areas were selected on each patient with stable non segmental vitiligo. The duration of treatment of volunteers was for 3 months starting with or without the topical application of bFGFRP followed by NBUVB on 30 patients. The results demonstrated that bFGFRP acted synergistically with NBUVB in repigmentation of the macules. More repigmentation occurred with NBUVB + bFGFRP at all-time points of evaluation (1, 2, and 3 months) than with NBUVB alone. NBUVB+ bFGFRP was superior to NBUVB alone in repigmenting vitiligo macules (23). Thus, it is clearly demonstrated that bFGFRP can be successfully used by itself or with synergistic effect in combination with many other modalities of treatment to treat vitiligo.
Discussion
We postulated that melanocyte growth factors are involved in repigmenting vitiligo macules (3). This theory was based on the observation that growth defects in vitiligo melanocytes could be corrected in successfully repigmenting vitiligo macules treated with PUVA and that the serum from such patients increased the proliferation rate of melanocytes obtained not only from untreated vitiligo subjects but also from normal subjects as shown in Table1. Later studies indeed showed that melanocyte growth factors in the serum of PUVA treated patients increased particularly bFGF by more than 3-fold compared to normal (24).
However, the role of growth factors in the etiology of vitiligo and repigmentation of vitiligo macules was not appreciated till recently (5, 24). The prominent theories on etiology of vitiligo have been on the loss of melanocytes /death of melanocytes by oxidative stress and of auto immune theories (1). It was demonstrated that vitiligo melanocytes are more prone to oxidative stress than normal melanocytes (2). The oxidative stressed melanocytes express on their membranes calreticulin protein which elicits immune reaction leading to its apoptosis (immunogenic apoptosis (4). Also, there are many reports demonstrating that keratinocytes in vitiligo also are abnormal, and they also die by apoptosis (25). This in turn leads to deprivation of growth factors particularly bFGF to melanocytes.Lotti et al (5) suggested that high levels of reactive oxygen species (26) in vitiligo contribute to structural damage affecting the keratinocyte- melanocyte crosstalk which is a key factor for correct skin pigmentation (5).Thus, it is clear that the independent theories of oxidative stress, and autoimmune theories are now interlinked with vitiligo melanocyte being more prone to oxidative stress and the oxidative stressed melanocyte having more calreticulin on their membranes eliciting an immune response leading to its death (2,4).The conclusions of these studies (2) may have limitations(27). But the fact that the level of serum HO-1 was signi?cantly decreased and that of IL-2 was markedly increased in 113 vitiligo patients when compared with healthy controls could overcome the expressed limitations (27) on its conclusions) (2). Moreover, the results presented by Z.Jian et al (2) are in line with the ideas expressed in recent publications (4, 5). At the same time, vitiligo keratinocytes are also damaged by oxidative stress (5,25) affecting the crosstalk between keratinocytes and melanocytes essential for correct epidermal pigmentation by way of signaling growth factors particularly bFGF which control physiological melanocytes proliferation, their migration (28), and proper melanin production (29). Growth factor deprivation theory as a possible cause of vitiligo (3) is in the light of the present literature mentioned above intimately intertwined with other prevailing theories of oxidative stress and auto immune theories (5). These theories are not mutually exclusive but interrelated and all together contribute to the loss of melanocytes resulting in vitiligo. The most important event that results in the initiation of repigmentation of vitiligo macule by any treatment modality is the proliferation of melanocytes as a result of increase in melanocyte mitogens (3, 11, and 24) and their migration towards the interior and center of the vitiligo macule. Migration of the melanocytes is a result of bFGF (28) whose level increases after the treatment (3, 11, and 24). Therefore, the present treatment with bFGFRP described in this chapter is to supplement this process by external application of active mitogen to induce proliferation of melanocytes and their migration towards the centre of the depigmented vitiligo lesion. In conclusion, the present treatment with bFGFRP described above is well-tolerated and effective by itself but also act synergistically with PUVASOL/PUVA, NBUVB, steroids or punch graft surgery or other surgical procedures to treat vitiligo. Acknowledgements: The author is grateful to Prof. Davinder Prasad of PGI Chandigarh who supervised the clinical trials while he was at Himalayan Institute of Medical Sciences Jolly Grant with deca peptide lotion alone,PUVASOL with and without deca peptide lotion and with oral mini pulse therapy with and without deca peptide lotion and Prof AS Kumar at Owaisi hospital Hyderabad who supervised the clinical trial with PUV-A+deca peptide lotion on vitiligo patches resistant to PUV-A alone and above all to all the volunteers who participated in the various clinical trials described herein.
References
1. Naresh C Laddha, Mitesh Dwivedi, Mohmmad S Mansuri, Amina R Gani, et al. (2013) Vitiligo: interplay between oxidative stress and immune system. Experimental Dermatology 22: 245–250.
2. Zhe Jian, Kai Li, Pu Song, Guannan Zhu, Longfei Zhu, et al. (2014) Impaired Activation of the Nrf2-ARE Signaling Pathway Undermines H2O2-Induced Oxidative Stress Response: A Possible Mechanism for Melanocyte Degeneration in Vitiligo. Journal of Investigative Dermatology 134: 2221–2230.
3. Ramaiah A, Puri N, Mojamdar M (1989) Etiology of vitiligo: A new Hypothesis. Acta Derma Venereol 69: 323-326.
4. Yajun Zhang, Ling Liu1, Liang Jin, Xiuli Yi1, Erle Dang, et al. (2014) Oxidative Stress–Induced Calreticulin Expression and Translocation: New Insights into the Destruction of Melanocytes. Journal of Investigative Dermatology 134: 183–191.
5. Lotti T, Hercogova J, and Fabriji G (2015) New therapeutic opportunities in Dermatology: Low dose Cytokine treatment for vitiligo. Jour Pigmentary disorders 3: 001-3.
6. Hussain I, Vijayan E Ramaiah A, Pasricha JS, Madan N (1982) Demonstration of tyrosinase in the vitiligo skin of human beings by a sensitive fluorometric method as well as by 14C (U) –L-tyrosine incorporationin to melanin. J Invest. Dermatol 78: 243-2527.
7. Tobin JD, Swanson NN, Pittelkow RM, Peters ME, Schallreuter UK et al. (2000) Melanocytes are not absent in lesional skin of long duration vitiligoJ. Pathol 191: 407-16.
8. Sehgal VN, Srivastava G (2007) Vitiligo: Compendium of clinico-epidemiological features. Indian J Dermatol Venereol Leprol 73: 149-56.
9. Alain Taïeb, Mauro PicardoN Eng (2009) Clinical practice. J Med; 360: 160-169.
10. Ramaiah A (2000) Pigmentary agent US patent N0:6143723.
11. Puri N, Mojamdar M, Ramaiah A (1987) In vitro growth characterstics of melanocytes obtained from adult normal and vitiligo subjects, J. Invest Dermatol 88: 434-438.
12. Mojamdar M, Puri N, Ramaiah (1987) An Effect of mitogenic factors extracted from fetal lung fibroblasts on the in vitro growth of melanocytes obtained from normal and vitiligo subjects. Journal of Biosciences; 11: 399-407.
13. N Puri, M Mojamdar A Ramaiah, (1989) Growth defects of melanocytes in culture from vitiligo subjects are spontaneously corrected in vivo in repigmenting subjects and can be partially corrected by the addition of fibroblast-derived growth factors in vitro. Arch Dermtol.Res, 28: 178-184.
14. Medrano EE Norduland JJ (1990) Successful culture of adult human melanocytes obtained from normal and vitiligo donors. J. Invest. Dermatol 95: 441-445.
15. Riley PA (1969) Hydroxyanisole depigmentation: in-vivo studies. J Pathol 97: 185-191.
16. Ramaiah A, A composition capable of administering an active agent, Patent IN 186437.
17. Kumar YL, Yadav M (2002) Guinea pig model for pre-clinical therapeutic evaluation of treatment modalities in vitiligo. 18th Iinternational Pigment Cell Conference Pigment Cell Res 15: 45.
18. Westerhof Wiete,Ludmila Nieuwebor-krobotova, Treatment of vitiligo with UV-B radiation VS topical psoralenPlus UV-A, Arch.Dermatol (!997) 186, 1525-1528.
19. Henseler T, Cristopher E, Honigsmann H, Wolff K (1997) Skin tumors in European PUV-A study, 8 year follow up of 1643 patients treated with PUV-A for psoriasis, J Am Acad Dermatol 16: 108-116.
20. Stern RS, Lard M, (1994) The carcinogenic risk of treatment for severe psoriasis. Photochemotherapy follow up study 73: 2759-2764.
21. Pasricha, JS, Khaitan, BK (1993), Oral minipulse therapy with betamethasone in vitiligo patients having extensive or fast spreading disease. Int, Jour Dermatol 32: 753-757.
22. P Kamala Subhashini, Dr K Sankar, Dr. Chandrakala Kambar, Dr V VenkataRamana (2015) Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861. 14: 41-47.
23. Ramaiah A, Kar HK, Garg VK, Bajaj N, Gupta L, et al. (2015) A Double-Blind Randomized Phase IV Clinical Trial of basic Fibroblast Growth Factor Related Deca-peptide in Vitiligo. Pigmentary Disorders 3: 3-004.
24. Wu CS, Lan CC, Wang LF, Chen GS, Wu CS, et al. (2007) Effects of psoralen plus ultraviolet A irradiation on cultured epidermal cells in vitro and patients with vitiligo in vivo. Br J Dermatol 156: 122-129.
25. Lee AY, Kim NH, Choi WI, Youm YH (2005) Less keratinocyte-derived factors related to more keratinocyte apoptosis in depigmented than normally pigmented suction-blistered epidermis may cause passive melanocyte death in vitiligo. J Invest Dermatol 124: 976-983.
26.Kostyuk VA, Potapovich AI, Cesareo E, Brescia S, Guerra L, et al. (2010) Dysfunction of glutathione S-transferase leads to excess 4-hydroxy-2-nonenal and H (2)O(2) and impaired cytokine pattern in cultured keratinocytes and blood of vitiligo patients. Antioxid Redox Signal 13: 607-620.
27. Lei Qiu, Zhiqi Song, Vijayasaradhi Setaluri (2014) Oxidative Stress and Vitiligo: The Nrf2-ARE Signaling Connection. J Invest Dermatol 134: 2074–2076.
28. Horikawa T, Norris DA, Yohn JJ, Zekman T, Travers JB, et al. (1995) Melanocyte mitogens induce both melanocyte chemo kinesis and chemo taxis. J Invest Dermatol 104: 256-259.
29. Puri N, Mirjan B, Vanderweel, Freck S de wit, Syad S Asghar et al. (1996) Basic fibroblast growth factor promotes melanin synthesis by melanocytes. Arch.Dermtol.Res 288: 633-635.