A Case of Bilateral Retinal Detachment in A Pregnant Patient with Severe Preeclampsia
Maria Maricar A. Manuel1*
1 Far Eastern University-Nicanor Reyes Medical Foundation, Quezon City, Philippines.
*Corresponding Author: Maria Maricar A. Manuel, Far Eastern University-Nicanor Reyes Medical Foundation, Quezon City, Philippines, Tel: +63 926 460 3040; Fax: +63 926 460 3040; E-mail: manuel.mmam@aol.com
Citation: Maria Maricar A. Manuel(2022) A Case of Bilateral Retinal Detachment in A Pregnant Patient with Severe Preeclampsia.Int Ginecolgia obstcia2:112.
Copyright: © 2022 Maria Maricar A. Manuel, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 18, 2022; Accepted: May 28, 2022; Published: June 01, 2022.
Abstract
Exudative retinal detachment is an unusual cause of visual loss in Preeclampsia. The visual system may be affected with variable intensity, being the retinal detachment a rare complication [1]. We report a case of 30-year-old Myopic, Term Primigravid with Severe Preeclampsia who developed bilateral exudative retinal detachment at the time of labor. Labor was induced due to low amniotic fluid volume and subsequently reached second stage of labor. She underwent emergency Low Segment Cesarean Section I due to Prolonged Second Stage of Labor secondary to Cephalopelvic Disproportion at the level of the midplane. Preeclampsia, Myopia and maternal exhaustion could have been contributed to the development of bilateral retinal detachment in this patient. She was co-managed with Ophthalmology Retina Service was given oral and topical Steroids and advised strict blood pressure monitoring and control. Two weeks after delivery, there was spontaneous and complete resolution of the bilateral exudative retinal detachment, with residual pigmentary changes of the retinal pigment epithelium. The management of retinal detachment as a complication in preeclampsia is conservative and the prognosis is usually good.
Keywords
Keywords: Preeclampsia, Retinal Detachment, Myopia.
Introduction
Preeclampsia is classified as a hypertensive disorder in pregnancy, which occurs in the absence of other causes of elevated blood pressure and in combination with generalized edema, proteinuria or both. Preeclampsia occurs in 5% of first pregnancies and underlying abnormality is thought to be severe generalized vasospasm occurring throughout the body as a result of increased sensitivity to circulating prostaglandins. The visual system may be affected in 30-100% of patients with preeclampsia. Serous retinal detachment is an unusual, cause of visual loss in preeclampsia, being produced by the involvement of the choroidal vascularization. This complication occurs in less than 1% of preeclamptic patients, with a slightly higher incidence in eclamptic patients [2,3].
Preeclampsia is an obstetric disease of unknown cause that affects approximately 5% of pregnant women. It is a systemic disorder that can affect almost every organ in the body. It is associated with increased rates of maternal morbidities such as pulmonary edema, cerebral edema and hemorrhage, acute renal failure, disseminated intravascular coagulopathy, abruptio placentae, liver hemorrhage or rupture, adult respiratory distress syndrome, sepsis, stroke, and retinal detachment. The visual system may be affected with variable intensity, being the retinal detachment a rare complication. The retinal detachment in preeclampsia is usually bilateral and serous, and its pathogenesis is related to the choroidal ischemia secondary to an intense arteriolar vasospasm. The majority of patients have complete recovery of vision with clinical management, and surgery is unnecessary [1,3]. This reports a case of bilateral exudative retinal detachment in a 30-year-old woman at term who developed preeclampsia during her first pregnancy and complained of worsening blurring of vision described as vision of being underwater, obscuring her sight.
Objectives
General Objective: To present a case of a 30-year-old Myopic, Term, Primigravida, who developed worsening blurring of vision during the course of her labor.
Specific Objectives: a. To discuss bilateral retinal detachment as a sequela of Preeclampsia; b. To identify the risk factors in the development of Bilateral Retinal Detachment; c. To review the appropriate management for such case.
Case Report
This is a case of a 30-year-old with Myopia, Gravida 1 Para 0, who was seen at 38 weeks and 3 days, with an ultrasound result of low amniotic fluid volume at 3.47 cm by Amniotic Fluid Index, and 1.49 cm by Single Vertical Pocket. On the first trimester of pregnancy, the patient experienced the usual signs and symptoms of pregnancy. On the first month of missed period, pregnancy test was done and revealed a positive result. She then sought consult with a private obstetrician wherein Complete Blood Count and Urinalysis were done and was normal. She was prescribed with Multivitamins and Folic acid. Transvaginal Ultrasound was done for pregnancy evaluation and revealed a single, live, intrauterine pregnancy at 8 weeks and 1 day. She had no exposure to radiation, toxic chemicals or infection on her first trimester.
During the second trimester of pregnancy, quickening was felt on the 5th month. On her 25 weeks and 6 days Age of Gestation, she had her first prenatal check-up at our out-patient department. During this trimester, her blood pressure ranges from 110-120/70-80 mmhg. Her fundic height ranges from 26 cms on her first prenatal check-up at our out-patient department to 29 cms on her 28th week age of gestation. Other prenatal screenings tests were done and all revealed normal results. She was compliant with her prenatal medications. On her 6th month of pregnancy, Congenital Anomaly Scan was done and revealed a pregnancy at 25 weeks and 5 days, normohydramnios with Estimated Fetal Weight, appropriate for gestational age.
Figure 1: Fundoscopy, Right Eye. This is a picture of the dilated fundoscopic examination done on the patient on the right eye. The optic disk and the optic nerve that passes through the optic disk and the macula which is clearly delineated can be appreciated.
Figure 2: Fundoscopy, Left Eye. This is a picture of the dilated fundoscopic examination done on the patient on the left eye. The optic nerve can be clearly seen entering the disk, however, the macula appears hazy compared to the macula on her right eye.

Figure 3: Optical Coherence Tomography (OCT), Right Eye.
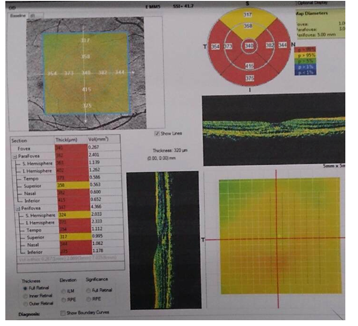
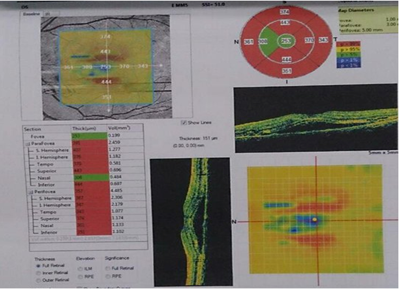
Figure 4: Optical Coherence Tomography (OCT), Left Eye.
During the third trimester of pregnancy, she had her regular prenatal check-up at our out-patient department with regular intake of prenatal medications, blood pressure ranges are within normal during her checkups. Maternal weight shows increasing trend from 54.3 kg on 30 weeks age of gestation up to 58 kg at 37 weeks age of gestation. Fundic height ranges from 29 cms at 30 weeks age of gestation up to 33 cms at 35 weeks age of gestation.
The history of present pregnancy started 5 hours prior to admission when the patient had her regular prenatal check-up at our out-patient department, with complaint of frequent uterine contractions occurring 7-8 contractions per hour, with no associated headache, blurring of vision, nausea, vomiting nor severe abdominal pain. She denies hypogastric pain, vaginal bleeding nor watery discharge with good fetal movement. On physical examination patient is conscious, coherent, not in cardiorespiratory distress with a note of an elevated Blood Pressure at 140/90 mmhg. Pertinent Physical Examination includes a fundic height at 28 cm, fundus occupied by breech, fetal back on the left, fetal small parts on the right, cephalic, with fetal heart tones of 130s-150s bpm best heard at the left lower quadrant, estimated fetal weight of 2,400-2,600 grams by clinical estimate. Internal examination revealed a normal-looking external genitalia, nulliparous introitus, vagina admits two fingers with ease, cervix is posterior in position, soft, and closed, cephalic, floating. Clinical pelvimetry revealed a sacral promontory not easily reached at 12 cm, sacrum deep and well-curved, sacrosciatic notch is average, ischial spines slightly prominent, side walls convergent and pubic arch average. Biophysical Score with Biometry was then requested and revealed a single, live intrauterine gestation at 34 weeks gestation by Biometry, Cephalic, with estimated fetal weight below the 10th percentile for age at 2,199 grams along with Oligohydramnios (Single Vertical Pocket of 1.49 cm and Amniotic Fluid Index of 3.47 cm) with grade III, high lying placenta. Because of abnormal ultrasound result, patient was subsequently admitted.
The admitting diagnosis was Gravida 1 Para 0, Pregnancy Uterine 38 weeks and 3 days, Cephalic not in Labor, Gestational Hypertension, Oligohydramnios, T/C Intrauterine Growth Restriction. Our first identified problem in our patient was her Gestational Hypertension. During her previous prenatal check-ups at our out-patient department, her blood pressure ranges were normal. However, on her latest consult, she had an elevated blood pressure at 140/90 mmhg. Therefore, upon admission, hypertensive work up was requested. Complete Blood Count, Creatinine, SGPT, Serum Potassium and LDH were within normal limits while Urinalysis showed proteinuria with +2 on dipstick urine. With the blood pressure of 140/90 mmHg and presence of proteinuria, she was then diagnosed to have Preeclampsia without severe features, hence, referred to the Perinatology service. The presence of preeclampsia links the other identified problems in this patient. Due of the presence of preeclampsia >37 weeks age of gestation, oligohydramnios and intrauterine growth restriction, our plan was for induction of labor. Prior to which, contraction stress test was done and revealed a negative result with baseline fetal heart tones of 130- 135 bpm, moderate variability, with accelerations, no decelerations, with note of 2 contractions in a 10-minute strip, moderate, 6 minutes apart lasting for 30-40 seconds. The bishop score of this patient was 2/10, hence, making her cervix unfavorable for induction. The service team decided to use Dinoprostone gel (Prostaglandin E2) for cervical ripening prior to induction of labor.
On the 12th hour of admission, her blood pressure remained 140/90 mmhg and repeat internal examination was done and revealed a closed cervix, beginning effacement, posterior, intact bag of waters, cephalic, station -1. With a CTG category I tracing, the second dose of Dinoprostone gel was then administered. However, 30 minutes after Dinoprostone gel was given, CTG Category II tracing was noted with baseline fetal heart tones of 140-145 bpm, moderate variability, no accelerations with recurrent variable decelerations with contractions occurring every 2-5 minutes, moderate lasting for 30-60 seconds. Because of this, the Dinoprostone gel was gently washed off and internal resuscitation was initiated by hydration with 200cc of D5LR, Oxygenation with O2 at 5 Lpm and she was maintained on left lateral decubitus. On her 15th hour from the 1st dose of Dinoprostone, internal examination was 1 cm cervical dilatation, beginning effacement, intact bag of waters, cephalic, station -1 with CTG Category I tracing. During this time at the 1st hour of labor, blood pressure was 150/90 mmhg and she complained of blurring of vision. Internal examination revealed 4 cm dilated cervix, 50-60% effaced, posterior, with intact bag of waters, cephalic, station -1. Perinatology service ordered Magnesium Sulfate loading dose 6g TSIV. On her 2nd hour of labor, blood pressure further elevated to 170/100 mmhg, now with progression of the blurring of vision described as vision of being underwater. CTG at Category I and Hydralazine 5mg TSIV was given. Repeat blood pressure was 150/90 mmhg. Magnesium Sulfate drip was then started at 1gm/hr. Because of her blood pressure elevation >160/110 mmhg, along with visual disturbances, she was now classified as Preeclampsia with severe features. Due to the presence of blurring of vision, she was referred to the Ophthalmology service wherein findings at that time was unremarkable. On the 3rd hour of labor, internal examination revealed to be 4 cm dilated, 50% effaced, intact bag of waters, cephalic, station -1. On the 4th hour of labor, uterine contractions were noted to be irregular every 11 minutes, moderate, lasting for 40-50 seconds, hence, Oxytocin drip was started at 12 gtts/min and titrated accordingly. On the 8th hour of labor, repeat internal examination revealed 5 cms dilated cervix, 50% effaced, intact bag of waters, cephalic, station -1, with uterine contractions occurring every 2-12 mins, strong, lasting for 30-50 seconds, hence, Oxytocin drip was titrated up to 16 gtts/min. At the 10th hour of labor, repeat internal examination revealed 6 cms, 60% effaced, intact bag of waters, cephalic station -1. Further titration of Oxytocin drip was done up to 20 gtts/min until regular uterine contractions were every 2-3 minutes, strong, lasting for 50-70 seconds were appreciated. At 11th hour of labor, the bag of waters spontaneously ruptured and revealed clear amniotic fluid with cervical dilatation at 7 cm, 60% effaced, ruptured bag of waters, right occiput posterior at station -1. At 12th hour of labor, cervix was 9 cms dilated, 80% effaced, ruptured bag of waters, occiput posterior at station +1. At 13th hour of labor, cervix was fully dilated, fully effaced, ruptured bag of waters, still at occiput posterior at station +1. Maternal pushing was started, however, after 3 hours of second stage of labor, the internal examination findings remained the same. She was the diagnosed with prolonged second stage of labor secondary to arrest in fetal head descent probably due to cephalopelvic disproportion-midplane. Hence, she underwent emergency low segment cesarean section I and delivered to a term baby girl, APGAR Score of 9 and 10, birth weight of 2,230 grams, asymmetrically small for gestational age.
On her post-operative day 1, blood pressure ranges were 130-150/80-90 mmhg, still with blurring of vision described as vision of being underwater with brown spots. Pertinent physical findings at that time were periorbital edema with pale palpebral conjunctiva, pinkish lips and palms. The Magnesium Sulfate drip was discontinued after 24 hours and because of the persistence of the blurring of vision, she was referred back to Ophthalmology service. Repeat complete blood count revealed anemia with hemoglobin of 84 mg/dL and was corrected with 2 units packed red blood cell. Serum postassium revealed a normal result and the 24-hour urine albumin result was elevated at 909.98 mg/day, further supporting the diagnosis of Preeclampsia. Dilated fundoscopic examination was done by Ophthalmology service with an impression of Bilateral Exudative Retinal Detachment; Periorbital Edema secondary to Preeclampsia, hence, was further referred to the Retina service. Visual acuity at this time on the left eye was 20/150. On the right eye, the optic disk and the optic nerve that passes through the optic disk and the macula which is clearly delineated were appreciated. In contrast to the the left eye, the optic nerve can be clearly seen entering the disk, however, the macula appears hazy compared to the macula on her right eye. A thorough Ophthalmologic examination in the form of Optical Coherence Tomography was done. Optical Coherence Tomography is a non-invasive imaging test that uses light waves to take cross-section pictures of the retina. pointed by the red arrow is the subretinal space of the left eye in comparison with the right, it contains fluid collection, hence, a subretinal edema. With these findings, along with an exudative retinal detachment she was collectively diagnosed as having hypertensive choroidopathy. She was started on Steroid therapy in the form Prednisone 60 mg 1 tab once a day and advised strict control of blood pressure. Irbesartan + Hydrochlorothiazide once a day in the morning and Amlodipine 10 mg 1 tab once a day in the evening were started.
On her 7th post-operative day, she was discharged with home medications such as Cefuroxime 500 mg 1 tab twice a day to complete for 7 days, Tramadol + Paracetamol 1 tab every 8 hours as needed for pain, Prednisone 60 mg 1 tab once a day in the morning, Irbesartan + Hydrochlorothiazide 1 tab once a day in the morning, Amlodipine 10 mg 1 tab once a day in the evening. Daily blood pressure monitoring twice a day was also advised. Final Diagnosis was Gravida 1 Para 1 (1001); Term, Cephalic, Delivered, Prolonged Second Stage of Labor-Arrest in Fetal Head Descent, Cephalopelvic Disproportion-Midplane; Low Segment Cesarean Section I (Intrapartum) under Combined Spinal Epidural Anesthesia; Term Birth, Living Girl, APGAR Score of 9 and 10, Birth weight of 2,230 grams, Asymmetrically Small for Gestational Age; Preeclampsia with Severe Features; Bilateral Exudative Retinal Detachment-Resolved; Hypertensive Choroidopathy.
On her consecutive weekly follow up at our out-patient department, her blood pressure ranges were 120-130/80-90 mmhg. In comparison from her visual acuity on her post operative day 2, 1 week post-operative shows a dramatic improvement on her visual acuity. The left eye was noted to be improved from 20/150 to 20/60. Her right eye also showed improvement from 20/70 to 20/50. At this point, Prednisone was discontinued and antihypertensive medications now include only Amlodipine 10 mg 1 tab once a day. She was allowed to resume breastfeeding. On her 2nd week post-operatively, her visual acuity further improved to 20/30 mmhg and she feels that her vision was just like before.
Case Discussion
We are presented with a case of a 30-year-old with Myopia, Gravida 1 Para 0, who was seen at 38 weeks and 3 days, with an ultrasound result of low amniotic fluid volume at 3.47 cm by Amniotic Fluid Index, and 1.49 cm by Single Vertical Pocket. The patient presented with increased blood pressure at 140/90 mmHg and a +2 protein in dipstick urine, hence, the diagnosis of Preeclampsia. Preeclampsia affects about 5% of all pregnancies, and is classically defined as the new onset of hypertension and proteinuria after the 20th week of gestation [2]. The onset of preeclampsia is often insidious and asymptomatic, but may include headache, visual disturbances, epigastric pain, weight gain, and edema of the hands and face. These early signs and symptoms are important to recognize clinically, since they may herald progression to more severe, often life-threatening, disease. Severe complications of preeclampsia can include acute renal failure, cerebral edema, cerebral hemorrhage, seizures (eclampsia), pulmonary edema, thrombocytopenia, hemolytic anemia, coagulopathy, and liver injury—including the syndrome of hemolysis, elevated liver enzymes, and low platelets (HELLP). Although antihypertensive medications help to lower blood pressure and magnesium sulfate is effective in seizure prophylaxis, delivery remains the only definitive treatment. When preeclampsia threatens to lead to severe maternal complications, urgent delivery of the fetus and placenta are often undertaken to preserve maternal health. Preeclampsia is associated with placental hypoperfusion, which can lead to intrauterine growth restriction and oligohydramnios, both present in the patient [2-4].
Table 1: Complete Blood Count.
|
Result |
Reference Range |
|
|
RBC |
|
|
|
Hemoglobin |
125 g/L |
120-140 |
|
Hematocrit |
0.404 L/L | 0.370-0.470 |
|
Platelet count |
240 x 10^9/L |
160-380 |
|
WBC |
11.62 x 10^9/L | 5.00-10.0 |
|
Neutrophils |
0.708 | 0.550- 0.650 |
|
Lymphocytes |
0.229 | 0.250-0.350 |
|
Monocytes |
0.054 | 0.020-0.060 |
|
Eosinophils |
0.008 | 0.030-0.050 |
|
Basophils |
0.001 | 0.000-0.010 |
Table 2: Urinalysis.
|
|
|
|
Color |
yellow |
|
Character |
hazy |
|
pH |
6.0 |
|
Specific gravity |
1.025 |
|
Protein |
+2 |
|
Glucose |
Negative |
|
Ketone |
Negative |
|
Blood |
+1 |
|
Leukocytes |
Negative |
|
Pus cells |
2-4 cells/hpf |
|
RBC |
2-3 cells/hpf |
|
Epithelial cells |
moderate |
|
Bacteria |
Few |
Table 3: Blood Chemistry.
|
Creatinine |
56.00 umol/L |
NV: 44-80 umol/L |
|
SGPT |
10.10 U/L |
NV: 11.20 U/L |
|
Potassium |
4.33 mmol/L |
NV: 3.50-5.10 mmol/L |
|
LDH |
220 U/L |
NV: 135-214 U/L |
Table 4: Visual Acuity.
|
LEFT EYE |
RIGHT EYE |
|
|
Post-operative Day 2 |
20/150 |
20/70 |
|
Post-operative Week 1 |
20/60 |
20/50 |
|
Post-operative Week 2 |
20/30 |
20/30 |
Oligohydramnios is a deficient volume of amniotic fluid. It is associated with maternal and fetal complications. Diagnosis is by ultrasonographic measurement of amniotic fluid volume. Management involves close monitoring and serial ultrasonographic assessments. The AFI is the sum of the vertical depth of fluid measured in each quadrant of the uterus [2]. The normal AFI ranges from 5 to 24 cm; values < 5 cm indicate Oligohydramnios. Such as in our case, the Amniotic Fluid Index was only 3.47 cm. Intrauterine growth restriction (IUGR) describes a fetus whose estimated weight is below the 10th percentile for its gestational age and whose abdominal circumference is below the 2.5th percentile [2]. Such as in our case, at 34 weeks age of gestation, the estimated fetal weight is below the 10th percentile for age at 2,199 grams. IUGR carries an increased risk of perinatal mortality and morbidity. Identification of IUGR is crucial because proper evaluation and management can result in a favorable outcome. Certain pregnancies are at high risk for growth restriction, although a substantial percentage of cases occur in the general obstetric population. Accurate dating early in pregnancy is essential for a diagnosis of IUGR. Ultrasound biometry is the gold standard for assessment of fetal size and the amount of amniotic fluid. Growth restriction is classified as symmetric and asymmetric. A lag in fundal height of 4 cm or more suggests IUGR. Serial ultrasonograms are important for monitoring growth restriction, and management must be individualized. General management measures include treatment of maternal disease, good nutrition and institution of bed rest. Preterm delivery is indicated if the fetus shows evidence of abnormal function on biophysical profile testing. The fetus should be monitored continuously during labor to minimize fetal hypoxia. Fetal growth restriction is the second leading cause of perinatal morbidity and mortality, followed only by prematurity. The incidence of intrauterine growth restriction (IUGR) is estimated to be approximately 5 percent in the general obstetric population. However, the incidence varies depending on the population under examination (including its geographic location) and the standard growth curves used as reference. In assessing perinatal outcome by weight, infants who weigh less than 2,500 g (5 lb, 8 oz) at term have a perinatal mortality rate that is five to 30 times greater than that of infants whose birth weights are at the 50th percentile. The mortality rate is 70 to 100 times higher in infants who weigh less than 1,500 g (3 lb, 5 oz). Perinatal asphyxia involving multiple organ systems is one of the most significant problems in growth-restricted infants [3,4].
Upon admission, the patient was not in labor with an internal examination of 1 cm cervix, posterior in position, soft, and closed, cephalic, floating. Because of these finding, the plan for this patient was for induction of labor. Labor induction is the stimulation of uterine contractions during pregnancy before labor begins on its own to achieve a vaginal birth. In the 1960s, Dr. Edward Bishop developed a pelvic scoring system to determine the likelihood of a woman going into labor in the immediate future. The score takes into consideration different factors of the cervix, and the fetal position, cervical dilation, cervical effacement, cervical consistency, cervical position and fetal station. The bishop score of this patient was less than 6, hence, making her cervix unfavorable for induction. The service team planned for cervical ripening prior to induction of labor. Dinoprostone gel (Prostaglandin E2) was used as the ripening agent and as well as for induction.
On her 15th hour from the 1st dose of Dinoprostone, internal examination was done with a note of 1 cm cervical dilatation, beginning effacement, intact bag of waters, cephalic, station -1 with CTG Category I tracing. However, on the 1st hour of labor, her blood pressure was 150/90 mmhg and she complained of blurring of vision during this time. On her 2nd hour of labor, blood pressure further elevated to 170/100 mmhg, now with progression of the noted blurring of vision. CTG was noted to be still Category I and Hydralazine 5mg TSIV was given. Repeat blood pressure was 150/90 mmhg. Magnesium Sulfate drip was then started at 1gm/hr. Because of her blood pressure elevation >160/110 mmhg, along with visual disturbances, she was now classified as Preeclampsia with severe features. Due to the presence of blurring of vision, she was referred to the Ophthalmology service wherein findings at that time were unremarkable. Due to the presence of blurring of vision and elevated systolic blood pressure of >160 mmHg, she was now diagnosed with Preeclampsia with severe features. Patients with preeclampsia with severe features display end-organ effects and may have the following signs and symptoms: headache, visual disturbances, altered mental status, blindness, dyspnea, edema, epigastric or right upper quadrant abdominal pain, weakness or malaise, clonus. Delivery is the definitive management for preeclampsia. Patients with preeclampsia without severe features are induced after 37 weeks' gestation.
In patients with preeclampsia with severe features, induction of delivery should be considered after 34 weeks' gestation [2]. In these cases, the severity of disease must be weighed against the risks of infant prematurity. In the emergency setting, control of BP and seizures should be priorities. Women with preeclampsia with severe features who are managed expectantly must be delivered under the following circumstances: non-reassuring fetal testing including (non-reassuring non-stress test, biophysical profile score, and/or persistent absent or reversed diastolic flow on umbilical artery Doppler velocimetry), ruptured membranes, uncontrollable BP (unresponsive to medical therapy), oligohydramnios, with amniotic fluid index (AFI) of less than 5 cm, severe intrauterine growth restriction in which the estimated fetal weight is less than 5%, oliguria (
Differentials for blurring of vision include: refractive errors, hypertensive retinopathy, cortical blindness and retinal detachment. In Hypertensive Retinopathy, the effect of hypertension extends to involve the vasculature of the retina, choroids and optic nerve head. At the pathophysiologic level, the primary response of the retinal vasculature to systemic arterial hypertension is vascular narrowing. This response to an increased blood pressure leads to focal or diffuse vasoconstriction. In addition, extravasation of fluid to the extravascular spaces occurs as a result of increased vascular permeability. Resultant retinal changes may manifest as decreased retinal to vein ratio, cotton wool spots, hemorrhages, Elschnig spots and serous retinal detachments. Acute cortical blindness is one of the most dramatic presentations of preeclampsia and is historically known to be reversible. It is defined as blindness occurring in association with normal fundoscopy and pupillary function. It may result from cerebral vasospasm and ischemic injury or it may arise from vasogenic edema due to increased capillary permeability. Retinal Detachment is an unusual cause of visual loss in preeclampsia, first described by von Graefe in 1855. It involves separation of the neurosensory retina from the pigmented retinal epithelium (RPE) and is one of the emergency situations in ophthalmology.
Dilated fundoscopic examination was done by Ophthalmology service with an impression of Bilateral Exudative Retinal Detachment; Periorbital Edema secondary to Preeclampsia, hence, was further referred to the Retina service. Visual acuity at this time on the left eye was 20/150. On the right eye, the optic disk and the optic nerve that passes through the optic disk and the macula which is clearly delineated, were appreciated. In contrast to the the left eye, the optic nerve can be clearly seen entering the disk, however, the macula appears hazy compared to the macula on her right eye. A thorough Ophthalmologic examination in the form of Optical Coherence Tomography was done. Optical Coherence Tomography is a non-invasive imaging test that uses light waves to take cross-section pictures of the retina. pointed by the red arrow is the subretinal space of the left eye in comparison with the right, it contains fluid collection, hence, a subretinal edema. With these findings, along with an exudative retinal detachment she was collectively diagnosed as having hypertensive choroidopathy. She was started on Steroid therapy in the form Prednisone 60 mg 1 tab once a day and advised strict control of blood pressure. Irbesartan + Hydrochlorothiazide once a day in the morning and Amlodipine 10 mg 1 tab once a day in the evening were started.
The visual system may be affected in 30 to 100% of patients with preeclampsia. Blurred vision is the most frequent symptom, however, Retinal Detachment is a rare complication of Preeclampsia, affecting only 1 – 2% of patients with its severe form and 10% of those with Eclampsia [5]. It may be present either before or after delivery. Its rarity is further supported by Varghese et al, emphasizing that serous retinal detachment is a rare complication occurring in less than 1% of patients with Eclampsia, not even Preeclampsia. But how does retinal detachment occur in cases of preeclampsia? The main culprit in its pathophysiology is still vasospasm involving the terminal arterioles. With vasospasm, it leads to choroidal ischemia leading to the disruption of the retinal pigment epithelium. Because of the disrupted lining, proteins and fluid leak from the choriocapillaries into the subretinal space producing exudative retinal detachment [6]. In this case, she was started on prednisone. What would be the role of prednisone in retinal detachment? Studies show that steroids facilitate absorption of sub-retinal fluid and also reduce inflammation. Hypertensive choroidopathy typically occurs in young patients who experience an episode of acute hypertension associated with preeclampsia, eclampsia, pheochromocytoma or renal hypertension. This is associated with lobular non-perfusion of the choroidal capillaries that may lead to focal retinal detachment, while bilateral exudative retinal detachment may develop on very rare occasions. The patient also has Myopia or otherwise known as nearsightedness. Myopia occurs when the eye grows too long from front to back. Instead of focusing images on the retina (the light-sensitive tissue in the back of the eye), the lens of the eye focuses the image in front of the retina. People with myopia have good near vision but poor distance vision. The eyeball becomes elongated, therefore, causes thinning out of the eyeball wall, hence, increases the risk for retinal detachment. According to a journal by Dr. Thomas Burton, Myopia, Lattice Degeneration and Advancing Age are known to be important risk factors in retinal detachment disease, yet the extent to which each plays a role remains obscure. Approximately 20% of the United States population are myopic to some degree, whereas about 60% of detachments are associated with myopic refractive errors. It is suspected that patients with high degrees of myopia are at greater risk for detachment than patients with low or moderate degrees of myopia. Preeclampsia, Myopia and Stress due to maternal pushing for 3 hours, all therefore, contributed to the development of Bilateral Retinal Detachment in this patient.
On her consecutive weekly follow up at our out-patient department, her blood pressure ranges were 120-130/80-90 mmhg. In comparison from her visual acuity on her post operative day 2, 1 week post-operative shows a dramatic improvement on her visual acuity. The left eye was noted to be improved from 20/150 to 20/60. Her right eye also showed improvement from 20/70 to 20/50. At this point, Prednisone was discontinued and antihypertensive medications now include only Amlodipine 10 mg 1 tab once a day. She was allowed to resume breastfeeding. On her 2nd week post-operatively, her visual acuity further improved to 20/30 mmhg and she feels that her vision was just like before.
What made this case interesting is the importance of vision in a person’s life. Blindness can be prevented if we take into consideration the significance of baseline fundoscopy in all patients presenting with Preeclampsia.
Conclusion
• Preeclampsia is an obstetric disease of unknown cause that affects approximately 5% of pregnant women. The visual system may be affected with variable intensity, being the retinal detachment a rare complication.
• Preeclampsia, Myopia and the stress due to maternal pushing contributed together to the development of bilateral retinal detachment in this case as compared to patients with Preeclampsia alone.
• The majority of patients have complete recovery of vision with clinical management, and surgery is unnecessary.
Recommendation
Baseline Fundoscopy is very important and should be a routine part of the plan for the management of pregnancy-induced hypertension to detect early visual complications.
References
- Lee C, Hsu TY, Ou CY, Chang SY, Soong YK (1999) Retinal detachment in postpartum preeclampsia and eclampsia: report of two cases. Changgeng Yi Xue Za Zhi 22: 520-524. [crossref]
- Cunningham, Lenovo, Bloom, et al. (2014) Williams Obstetrics 24th edition, USA; 728-770
- Ober RR (1994) Pregnancy-induced hypertension (preeclampsia-eclampsia). In: Ryan SJ (ed). Retina. (2nd ed., vol. 2) St. Louis: Mosby; 1405-1411.
- Valluri S, Adelberg DA, Curtis RS, Olk RJ (1996) Diagnostic indocyanine green angiography in preeclampsia. Am J Ophthalmol122: 672-677. [crossref]
- Wang CL (1992) Exudative retinal detachment in the pregnancy-induced hypertension syndrome. Chang Hua Yen Ko Tsa Chih 2: 77-79.
- Bos AM, van Loon AJ, Ameln JG (1999) [Serous retinal detachment in preeclampsia]. Ned Tijdschr Geneeskd 143: 2430-2432. [crossref]