A Case of Tubal Schistosomiasis Presenting as a Ruptured Ectopic Gestation
Dineth Adrienne C. Gutierrez
1 Mary Johnston Hospital, Philippines
*Corresponding Author: Dineth Adrienne C. Gutierrez, Mary Johnston Hospital, Philippines, Tel: +63 2 8245 4051; Fax: +63 2 8245 4051; E-mail: dinethgutierrez@gmail.com
Citation: Dineth Adrienne C. Gutierrez(2022) A Case of Tubal Schistosomiasis Presenting as a Ruptured Ectopic Gestation.Int Ginecolgia obstcia2:109.
Copyright: © 2022 Dineth Adrienne C. Gutierrez, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: May 02, 2022; Accepted: May 14, 2022; Published: May 18, 2022.
Abstract
When Schistosomiasis, an infection caused by parasitic flatworms, involves the fallopian tubes, it produces fibrotic scars and tubal occlusion, leading to infertility and ectopic pregnancy [1]. While it is documented in areas with heavy worm burden, such as Africa and the Middle East, Schistosomiasis of the fallopian tube is rare, and presentation as an ectopic pregnancy in an asymptomatic patient is even more unusual [1].
A case of a 32-year-old primigravid from Northern Samar, with amenorrhea of 8 weeks and 5 days, who presented with vaginal spotting and hypogastric pain is hereby reported. She underwent salpingostomy for ectopic pregnancy and was later, upon histopathological examination, found to have tubal infection by Schistosoma, which was treated with Praziquantel. This case highlights tubal Schistosomiasis, despite its rarity in the Philippines, as a significant risk factor for ectopic pregnancy. Knowledge on this disease and a high index of suspicion is important in managing affected patients.
Keywords
Keywords: Ectopic Pregnancy, Praziquantel, Salpingostomy, Schistosomiasis, Tubal Schistosomiasis.
Introduction
Schistosomiasis is a tropical disease caused by parasitic flatworms of the genus Schistosoma that enter the human body through the skin. The different species of these schistosomes have predilections for specific organs in the body, and signs and symptoms depend on which areas are affected. Cases of Schistosomiasis of the female reproductive tract are rare but have been seen in areas of the world where Schistosoma haematobium, in particular, is endemic [1]. Thorough literature search at the Philippine Obstetrical and Gynecological Society (POGS) library revealed no reported local case of tubal Schistosomiasis to date. Furthermore, the only Schistosoma species that has been found in our country is Schistosoma japonicum [2], while the species most often isolated in tubal Schistosomiasis, in contrast, is Schistosoma haematobium [1].
This paper aims to discuss a case of Schistomiasis presenting as a ruptured tubal gestation. It is note-worthy because: a) no local case reports on tubal Schistosomiasis are currently available based on literature search; b) Schistosoma haematobium, the major species implicated in Schistosoma infection of the fallopian tube, is not found in the Philippines; and c) the finding of Schistosomiasis concomitant with a tubal pregnancy in a previously asymptomatic patient is quite rare [1,3].
Case Report
This is the case of M.B., a 32 year old married primigravid, Filipino, Christian, born and raised in Northern Samar, who came to our institution with a chief complaint of hypogastric pain. Three days prior to admission, the patient experienced sudden onset of hypogastric pain graded 5/10 on pain scale, crampy, non-radiating, associated with vaginal spotting. There was no associated fever, dysuria, or vaginal discharge. There was no history of trauma. There was no consult done nor medications taken. Symptoms persisted until a few hours prior to admission, when there was an increase in the severity of hypogastric pain, now graded 9/10, prompting consult at a local health center. A urine pregnancy test was done, which revealed a positive result. At the time, patient was non-cognizant of pregnancy but had been amenorrheic for 8 weeks and 5 days. The patient underwent transvaginal ultrasound, which revealed a normal- sized, anteverted uterus, a hyperechoic, thickened endometrium at 1.1 cm, normal bilateral ovaries, and a complex mass at the right adnexa measuring 5.3 x 6.7 x 4.1 cm with moderate fluid in the cul-de-sac, suggestive of a ruptured ectopic gestation. She was advised surgery, hence referral to our institution and subsequent admission.
Past medical history, family, and personal/social history were non-contributory. The patient had no previous surgeries or any pelvic infections. She had no recent travel. The patient had been regularly menstruating since 13 years of age and had her first sexual contact at 16 years old with one monogamous sexual partner. She denied having dyspareunia, post-coital bleeding, chronic pelvic pain, or foul-smelling vaginal discharge. She has been married for 10 years and is currently a primigravid of 8 weeks and 5 days age of gestation. Review of systems revealed no weight loss, no fever, no rash, no jaundice, no vomiting, no changes in bowel movement, no hematochezia, no dysuria or hematuria, and no edema. On physical examination, the patient was conscious, coherent, ambulatory, and not in distress with normal vital signs. The rest of the systemic findings were unremarkable. Focusing on the abdominal examination, there were no lesions or masses on inspection. Abdomen was flabby, soft, with normoactive bowel sounds, with direct and rebound tenderness on the right lower quadrant. Speculum examination revealed a smooth, violaceous cervix with minimal bleeding per os. Upon internal examination, the cervix was soft, closed, with wriggling tenderness. Corpus was small, and there was a palpable 5 x 4 cm solid, tender, movable right adnexal mass.
The initial assessment was Ectopic Pregnancy 8 weeks and 5 days age of gestation by last menstrual period, probably ruptured. Exploratory Laparotomy was done, wherein approximately 250 mL of hemoperitoneum with placenta-like tissues was evacuated. The ampullary area of the right fallopian tube was dilated to 2 x 3 cm with no point of rupture. The contralateral fallopian tube, both ovaries, and the uterus were grossly normal. With these findings, a Right Salpingostomy was done. The patient tolerated the procedure well. The rest of the patient’s hospital stay was uneventful and she was discharged stable and improved on the 4th hospital day.
On follow-up, the patient had no subjective complaints, with good wound healing at the post-operative site. Histopathological study of the patient’s surgical specimen, however, revealed Tubal pregnancy and Schistosomiasis (Histopathological Specimen, Figures 1 to 4). A referral to Gynecologic Infectious Service was made and the patient was started on Praziquantel therapy at a dose of 20 mg/kg thrice a day, done three weeks apart. One month after completion of treatment, the patient underwent Kato-Katz testing which revealed absence of helminthic ova or parasites. She was then considered treated and was advised to follow up as needed.
Figure 1: shows a scanner view of multiple chorionic villi, composed of the syncytiotrophoblast and cytotrophoblast, denoting the presence of pregnancy in this specimen obtained from inside the fallopian tube. Denuded epithelium of the fallopian tube, composed of simple columnar cells, are also seen. Lastly, at the lower portion of this photo is a single calcified parasitic ovum amongst red blood cells and areas of necrosis.
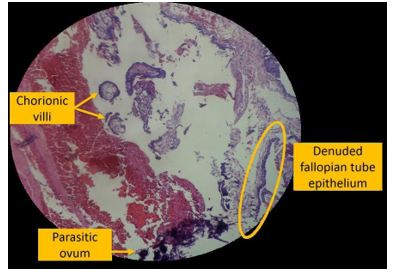
Figure 2: shows a magnified view of the chorionic villi, composed of an inner layer of cytotrophoblast and an outer layer of syncytiotrophoblast. Since this is an early first trimester placenta, it is devoid of blood vessels. The presence of chorionic villi in the specimen obtained from the fallopian tube provides evidence of pregnancy.
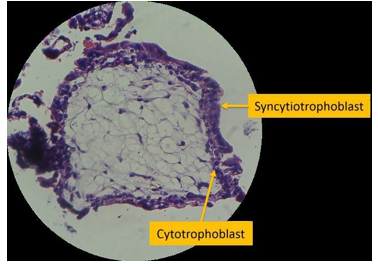
Figure 3: shows multiple parasitic ova embedded within a background of red blood cells and areas of necrosis and fibrosis.
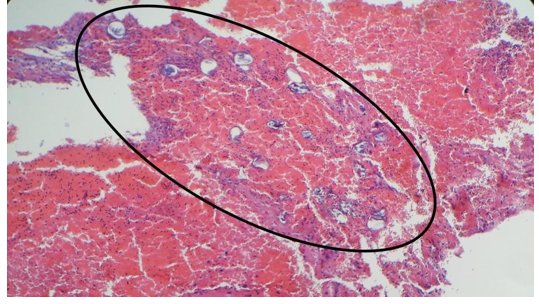
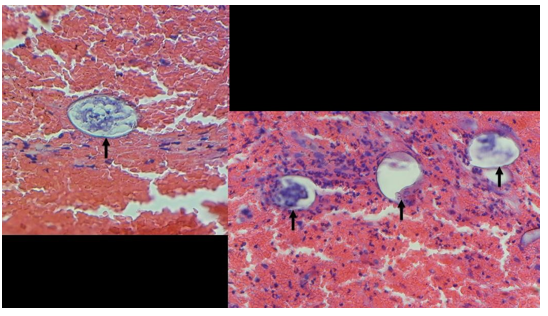
Figure 4: shows high-power views of Schistosoma eggs found in different parts of the specimen, surrounded by red blood cells and infiltrates. The egg is seen to be oval-shaped, with no visible terminal or lateral spine on its shell. This appearance is consistent with Schistosoma japonicum species, the only Schistosoma species found in the Philippines.
Case Discussion
Definition: Schistosomiasis, an infection caused by parasitic flatworms, was first described in Cairo in 1852 by Theodor Bilharz, hence its alternate name of Bilharziasis [4]. The World Health Organization (WHO) has placed this disease as the third most devastating tropical disease, outranked only by malaria and intestinal helminthiasis [2]. Also known as “snail fever”, transmission relies on its intermediate hosts comprised of certain types of freshwater snails. The infectious form of the parasite, known as cercaria, emerges from the snail, hence contaminating water. Humans then become infected once they come in contact with this water, as schistosomes penetrate the skin of persons who are wading, swimming, bathing, or washing [5,6]. Five species are widely known to infect humans, namely Schistosoma japonicum, Schistosoma mansoni, Schistosoma haematobium, Schistosoma intercalatum, and Schistosoma mekongi [2,4]. Schistosoma haematobiumcauses urinary Schistosomiasis while Schistosoma mansonicauses intestinal Schistosomiasis [7]. Tubal schistosomiasis is a granulomatous infection of the fallopian tubes caused by the body tissues’ inflammatory reaction to helminthic ova of Schistosoma haematobiumand Schistosoma mansoni, the former being the most common species isolated in this type of pathology [8].
Epidemiology: Schistosomiasis is endemic in 74 nations and affects over 240 million people worldwide [2,3,9]. In the Philippines, the Department of Health has stated that 28 provinces are still endemic for Schistosomiasis as of 2012 [2]. Among the five species affecting humans, only one, Schistosoma japonicum, is found in the Philippines [2], where it has major foci in the islands of Leyte, Samar, Mindanao, Negros Occidental, and Cagayan [2,3]. Schistosomiasis is dominant in tropical areas, especially in places with poor sanitation. School-aged children who live in these areas are most at risk because they tend to spend time swimming or bathing in water containing infectious larvae [6]. Our patient was born and raised in Northern Samar before moving to Manila at 11 years of age. According to prevalence studies done from 2005 to 2008, Northern Samar, an area surrounded by bodies of water, ranked fourth in the list of Philippine provinces endemic for Schistosomiasis, with a prevalence rate of 2.4% [10]. It is highly probable that our patient contracted Schistosoma infection during her childhood years living in this province.
Schistosomiasis of the female reproductive tract has been documented in areas of the world where Schistosoma haematobium is endemic, such as in Africa and the Middle East [1,7]. The epidemiology of tubal Schistosomiasis, however, is yet to be estimated because only cases with overt disease are usually considered [11]. In the same vein, the incidence of tubal ectopic gestation caused by schistosomiasis-induced tubal pathology remains undocumented, probably be due to the rarity of this pathology [7].
Clinical Presentation: The different signs and symptoms of Schistosomiasis are attributable to the three phases of this disease: 1) initial penetration of cercariae, which produces a pruritic, papular rash known as cercarial dermatitis or “swimmer’s itch” at the point of entry, 2) initiation of egg-laying which occurs a few weeks after skin penetration (acute schistosomiasis or Katayama fever), and 3) late stage complication of tissue proliferation and repair (chronic schistosomiasis) [4-6]. Focusing on the consequences of chronic Schistosomiasis on the female genital organs, the presence and lodging of Schistosoma ova in these areas can lead to symptoms such as lower abdominal pain, dysmenorrhea, dyspareunia, or bloody cervical discharge. Genital schistosomiasis can also complicate pregnancy, causing ectopic pregnancy, abortion, preterm labor, intrauterine growth retardation, and stillbirth [12]. Tubal involvement can produce fibrotic scars, tubal occlusion, and infertility [12]. In many cases, however, female genital Schistosomiasis remains asymptomatic [1].
Our patient was unable to recall any history of sudden onset of a pruritic rash or of a febrile illness during her childhood years in Northern Samar. Her parents likewise were unable to provide any information regarding such events. The patient also denied experiencing abdominal pain, menstrual abnormalities, or dyspareunia. There is, however, evidence of impaired fertility in this patient as she reported having had regular, unprotected sexual contact with her husband of 10 years, occurring 2 to 4 times a week, ever since she started co-habituating with him at 16 years of age, and yet she was unable to conceive and only had her first pregnancy 16 years later, which, as discussed, turned out to be ectopic. No consult was done for the infertility. With these indications of tubal involvement, it can be surmised that our patient is currently at the chronic stage of tubal Schistosoma infection.
Pathophysiology: Schistosomiasis of the female genital tract is predominantly caused by Schistosoma haematobium, occurring in 50 to 80% of parasitized women [12]. Surgicopathologic case reports done in patients with this disease revealed that Schistosoma haematobiumova can be found in all female genital organs, most commonly in the cervix and vagina but rarely in the fallopian tubes [12]. Adult male and female forms of these blood flukes, which reside in pelvic and vesical venous plexuses, gain access to the genital tract through natural venous anastomoses between the hemorrhoidal and hypogastric veins [9]. As the eggs penetrate the urinary system, they find their way to the female genital region and induce a granulomatous reaction (the Splendore-Hoeppli phenomenon) that leads to fibrosis and the side effects of female genital Schistosomiasis as previously discussed [11]. The pathophysiologic mechanism implicated in ectopic pregnancy associated with tubal Schistosomiasis is based on mechanical obstruction of the fallopian tubes by the body tissues’ granulomatous reaction to the trapped Schistosoma ova, with associated fibrosis and distortion of the tubes [12]. The thickened, damaged muscle layers of the fallopian tube cannot properly perform their function of propelling the fertilized ovum towards its proper destination, the endometrial lining of the uterus, and thus tubal implantation and infertility occur [13].
Diagnosis: A definitive diagnosis of Schistosomiasis requires demonstration of Schistosoma eggs in feces, known as the Kato-Katz technique, or in the urine by direct wet mount or formalin-ethyl acetate concentration methods, or in tissue obtained through biopsy [5,6]. Serologic tests using immunodiagnostic methods and purified worm antigens are used to screen travellers and immigrants from endemic areas. Quantitative assessment of stool and urine specimens is recommended to determine the intensity of an infection. However, these tests are unable to distinguish new from old infections. The active stage is epidemiologically important because of its role in transmission. It is during this stage where the destructive process can be dramatically altered by instituting chemotherapy, thus converting active into inactive disease [4,10]. Our patient was unable to undergo any type of screening or diagnostic method for Schistosomiasis while she was growing up in Northern Samar. She could have benefited from treatment had this covert infection been recognized earlier, thus stressing the need to better implement mass screening for Schistosoma infection in endemic areas.
Treatment: Treatment is indicated for all persons with Schistosomiasis. Praziquantel is acknowledged as the drug of choice for all Schistosoma species [14]. This drug causes spastic paralysis of the parasitic flatworms and damage to their outer tegument [14]. It notably kills the adult worm but does not affect the ova. The recommended dose for patients over 4 years of age is 20 mg/kg orally every 4 to 6 hours for one day, to be postprandially or a few minutes before a meal. Re-treatment can also be done after 2 to 6 weeks to increase cure rate. Praziquantel is well- tolerated and is well-absorbed, resulting in good serum levels. No serious toxicity is reported with this drug and it is also associated with a very low frequency of side effects, such as mild nausea and transient headaches. Success rates with Praziquantel have ranged from 90% to 100% in some studies for the total cure rate. Two second-line agents are available, depending on the species of Schistosoma involved: Metrifonate (10 mg/kg as single dose) for Schistosoma haematobium, and Oxamniquine (40-60 mg/kg as single dose) for Schistosoma mansoni. For Schistosoma japonicum, no second-line agent is available [14].
In the Philippines, mass treatment using Praziquantel has been a mainstay in the control program for Schistosomiasis [2]. The subsequent reduction in prevalence in many endemic areas resulting from mass treatment has encouraged the Department of Health to further pursue its goal in Schistosomiasis control, even pushing for elimination in some areas [2,6,10].
Summary
This case emphasizes that occurrence of tubal Schistosomiasis is possible, despite its rarity in the Philippines, and highlights this disease as a significant risk factor for ectopic pregnancy. Clinicians should thus consider Schistosomiasis as a differential diagnosis in patients presenting with signs and symptoms of ectopic pregnancy, especially in those from endemic areas, such as the patient in our case, or in those with history of travel to said regions.
Given its gynecological consequences as well as the additional morbidity associated with ectopic pregnancy, female genital Schistosomiasis should be of substantial public health importance in endemic countries. Furthermore, considering the diagnostic limitations of urine and stool microscopy, it is recommended that meticulous history-taking and complete parasitic evaluation should be considered an essential component of the management of patients presenting with ectopic pregnancy in areas where Schistosomiasis is endemic. The need for histopathological evaluation of surgical biopsies cannot be overemphasized, as illustrated by this case. This patient would have missed the opportunity for definitive treatment if the biopsy report had not been taken into account. Praziquantel therapy will treat the infection, though reversal of the tubal fibrosis and its sequelae cannot be assured. This highlights the need for long-term follow-up and counseling in such patients, especially if they are desirous of further pregnancies [15].
References
- Aminu M, Abduhalli K, Dattijo L (2014) Tubal ectopic gestation associated with genital schistosomiasis: A case report. African Journal of Reproductive Health18: 144- 146.
- Department of Health. National Schistosomiasis Control Program. Retrieved on March 7, 2016 from the DOH website.
- Olveda D, et al. (2014) Bilharzia in the Philippines: Past, present, and future. International Journal of Infectious Diseases 18: 52-56.
- Katsetos C, Kontoyannis M, Koumousidis A, Petroyannis N, Davies A, et al. (2013) Schistosomiasis of the abdominal cavity and infertility: A case report. OA Case Reports 2: 57-63.
- "Schistosomiasis Fact Sheet" (2016) World Health Organization. 3 February 2014.
- “Parasites–Schistosomiasis” (2016) Centers for Disease Control and Prevention.
- Faria C, Conceicao J, Valadares T, Rodrigues B, Carneiro L, et al. (2010) Schistosoma mansoni: A rare cause of tubal infection. Brazilian Journal of Infectious Diseases 14: 288-290.
- Ostrzenski A (2002) Gynecology: Integrating conventional, complementary, and natural alternative therapy. Lippincott Williams & Wilkins.
- Owusu-Bempah A, Odoi A, Dassah E (2016) Genital schistosomiasis leading to ectopic pregnancy and subfertility: A case for parasitic evaluation of gynaecologic patients in schistosomiasis endemic areas. Case Reports in Obstetrics and Gynecology.
- Leonardo L, Rivera P, et. al. (2012) A National Baseline Prevalence Survey of Schistosomiasis in the Philippines Using Stratified Two-Step Systematic Cluster Sampling Design. Journal of Tropical Medicine.
- Sahu L, Tempe A, Singh S, Khurana N (2013) Ruptured ectopic pregnancy associated with tubal schistosomiasis. J Postgrad Med59: 315-317.
- Odubamowo KH, Akinpelu OM, Lawal OO, Okolo CA, Odukogbe AA, et al. (2014) Bilateral tubal gestation associated with schistosomiasis in an African woman. Case Reports in Obstetrics and Gynecology 1-4.
- McFalls Jr JA, McFalls MH (1984). Studies in population: Disease and fertility. Academic Press, Inc.
- Sweet R, Gibbs R (2009) Infectious diseases of the female genital tract. Lippincott Williams & Wilkins.
- Kjetland E, Leutscher P, Ndhlovu P (2012) A review of female genital schistosomiasis. Trends in Parasitology 28: 58-65.
Appendix A
Surgical Pathology Report
Gross: The specimen submitted labelled “products of conception” consists of multiple pieces of dark brown, irregularly-shaped, rubbery tissues, with an aggregate measurement of 3.0 x 2.5 x 2.0 cm. Cut section shows smooth, solid, dark brown surface. All tissues embedded, 1 cassette.
Microscopic: No evidence of malignancy.
Diagnosis: Salpingostomy, right; • Tubal Pregnancy; • Schistosomiasis
Appendix B
Laboratory Results
a. Complete Blood Count
|
|
8/20/15 |
8/21/15 |
|
Hgb |
12.5 | 11.1 |
|
Hct |
35.5 | 32.0 |
|
RBC |
4.40 | 3.91 |
|
MCV |
80.7 | 81.8 |
|
MCH |
28.4 | 28.4 |
|
MCHC |
35.2 | 34.7 |
|
WBC |
10.16 | 16.59 |
|
Neut |
74.4 | 85.9 |
|
Lym |
19.5 | 8.6 |
|
Baso |
0.1 | 0.1 |
|
Mono |
5.2 | 5.3 |
|
Eos |
0.8 | 0.1 |
|
Plt |
306 |
243 |
|
MPV |
8.6 | 8.6 |
|
RDW-SD |
35.6 | 36.4 |
b. Urinalysis
|
|
8/20/15 |
|
Color |
Straw |
|
Characteristic |
Clear |
|
RBC |
1-3 |
|
WBC |
None found |
|
Crystals |
Calcium oxalate - few |
|
Epithelial Cells |
Few |
|
Bacteria |
None found |
|
Cast |
None found |
c. ABO w/ Rh typing: AB positive
d. Transvaginal Ultrasound
Uterus: 4.7 x 4.5 x 4.6 cm, anteverted, Endometrium: 1.1 cm thickness, hyperechoic.
Adnexae: Left Ovary: 2.6 x 2.5 x 2.7 cm, volume 9.8 cc, located lateral to the uterus, Right Ovary: Not visualized Within the right adnexa is a complex mass measuring 5.3 x 6.7 x 4.1 cm, probably representing an ectopic gestation.
Cervix: 3.0 x 2.5 x 1.9 cm, Others: (+) moderate fluid in the cul-de-sac.
Diagnosis: Normal-sized, anteverted uterus, Thickened endometrium, Normal left ovary, Right ovary not visualized, Complex mass, right adnexa, suggestive of ruptured ectopic gestation.