Methotrexate Induced Pancytopenia in a Patient with Rheumatoid Arthritis and Psoriasis: A Case Report.
Dr Bhoraniya Abdullah Ismail 1*, Dr Sayyed Asad 2, Dr Surekha Hoskeri 2
1Department of Moalajat (Medicine), National Research Institute of Unani Medicine for Skin Disorders, Opp. ESI Hospital, Eragadda, Hyderabad, 500038, India.
2 DNB (General Medicine)
2 MD (Respiratory Medicine)
*Corresponding Author:Dr Bhoraniya Abdullah Ismail, Department of Moalajat (Medicine), National Research Institute of Unani Medicine for Skin Disorders, Opp. ESI Hospital, Eragadda, Hyderabad, 500038, India, Tel: 00962795420286; Fax: 00962795420286; E-mail: abdullahismail519@gmail.com
Citation: Dr Bhoraniya Abdullah Ismail, Dr Sayyed Asad, Dr Surekha Hoskeri (2023) Methotrexate Induced Pancytopenia in a Patient with Rheumatoid Arthritis and Psoriasis: A Case Report. Cancer Prog Diagn 7: 135.
Received: March 20, 2023; Accepted: March 28, 2023; Published: April 3, 2023.
Abstract
Methotrexate (MTX) has an antiproliferative, anti-inflammatory, immunomodulatory, and immunosuppressive activity which is used in the treatment of many diseases such as Rheumatoid arthritis (RA), psoriasis, vasculitis, systemic lupus erythematosus, connective tissue diseases. This report describes the 2 cases of MTX-induced pancytopenia. Case 1; A 60-year-old female was having C/o loose motion 5-7 episodes for 2 days, severe generalized weakness, dark color stool, itchy rashes over the body, cheeks, inside the mouth, and buccal mucosa with RA, and was taking Tablet (Tab) Methotrexate 5 Mg on Saturday and Sunday, Tab Folic Acid 5mg once a day Monday to Friday for 3 months. The patient did not have a proper outpatient monitor of blood investigation resulting in toxicity. She was hospitalized, MTX withdrawn, and treated with folinic acid. Case 2; A 76-year male was admitted to Bombay port trust hospital with a chief complaint of bleeding from the groin region associated with burning, itching, pain, foul smell with skin maceration over the scrotum and penis, low back pain, severe generalized weakness, increased frequency of urination. The patient was case psoriasis on methotrexate for 1 year without a monitor of CBC, kidney, or liver function tests and had taken it continuously resulting in toxicity. He was hospitalized, MTX withdrawn, and treated symptomatically. Our case highlights the importance of counseling to ensure adherence to the correct MTX treatment regimen to prevent toxicity and its serious effects and a new alternative therapeutic method to treat autoimmune disease without measuring side effects and toxicity.
Keywords
Methotrexate, Overdose, Psoriasis, Pancytopenia, Rheumatoid Arthritis.
Introduction
Methotrexate (MTX) (4-amino-10-methyl folic acid) is a dihydrofolate reductase (DHFR) inhibitor, an analog, and an antagonist of folic acid. High-dose (HD) MTX (0.5 - 12 g/m2) has antiproliferative activity and is used in the treatment of cancer while low-dose (LD) MTX (10 - 40 mg/m2) has anti-inflammatory and immunosuppressive properties [1] [3]. By interfering with folate metabolism, methotrexate (MTX) impairs thymidine and DNA synthesis in rapidly dividing malignant cells, leading to cell death. MTX is primarily excreted by the kidneys (80%-90%) [2]. MTX is the first-line drug for the treatment of several rheumatic and non-rheumatic disorders. It is currently used as an anchor disease, modifying anti-rheumatic drug in the treatment of rheumatoid arthritis (RA). MTX is currently the first-line disease-modifying anti-rheumatic drug (DMARDs) in the treatment of RA, juvenile idiopathic arthritis, and psoriasis, and is useful in inflammatory bowel diseases, multiple sclerosis, vasculitis, systemic lupus erythematosus, connective tissue diseases, and transplantation [3]. Use of MTX associated Acute kidney injury (AKI) has been reported in 2% to 12% of patients receiving HDMTX while hepatic, pulmonary, and acute MTX toxicity presenting as a multiorgan failure and acute pneumonitis are rare [1-3].
Case Report 1
A 60 years old female patient was brought by a relative to Bombay port trust hospital, Mumbai. The patient was having Chief complaints of loose motions 5-7 episodes for 2 days, severe generalized weakness, dark color stool, itchy rashes over the body, cheeks, inside mouth, and buccal mucosa. On Examination patient was afebrile, Blood Pressure; 110/60mmhg, Pulse; 99/min, SPO2; 95% on room air. The patient was thin built and pallor was present. Systemic examination revealed cardiovascular system (S1, S2 audible, no murmurs), central nervous system (conscious, oriented in time, place, person, higher, motor, and sensory function intact), per abdomen (soft, no tenderness/guarding/ rigidity), respiratory system (Air Entry Bilaterally Equal, no added sound heard). The history of the patient revealed RA and was taking a Tablet (Tab) of Methotrexate 5 Mg on Saturday and Sunday, Tab of Folic Acid 5mg once a day Monday to Friday for 3 months. The patient did not have an outpatient monitor of CBC, kidney, or liver function tests. The patient was known to cause Diabetes Mellitus, Hypertension, and RA on treatment. No history of bronchial asthma, Chronic obstructive pulmonary disease, Cancer or Ischemic heart disease was present. Routine blood and Urine examination done showed in table 1. The patient was having pancytopenia which is found in several blood examinations as shown in table 1 which is intended to associate with methotrexate. Hematological examination revealed hypochromic, mild microcytosis, and anisocytosis RBC, with leukocytopenia. On admission patient's blood glucose; 130 mg/dl, urea;31, creatinine; 1.53, alt(pt); 19, bilirubin; 0.4mg/dl, sodium;133mg/dl, potassium;3.9mg/dl while at the time of discharge blood glucose; 146mg/dl, urea;26, creatinine; 1.27, alt(pt);11, bilirubin; 0.4mg/dl sodium;135mg/dl, potassium;4.2mg/dl. Chest X-ray and echocardiography were within normal limits.
Treatment Given
The patient was admitted to Intensive Care Unit. Temperature (T), Pulse(P), Respiratory Rate (RR), Blood Pressure (BP), SPO2, Input, and output chart maintained during the hospital course. No Intramuscular Injection was given. Intra Venous fluid, antibiotic (ceftriaxone 1gm BD), antiemetic (ondansetron 4mg TDS), antacid (pantoprazole 40mg OD) given for 5 days. Orally patient given Capsule Vyzylac BD 3 Day, oral hypoglycemic drugs, and anti-hypertensive drugs. Tab Hydroxychloroquine 200 BD, Tab Folic Acid 5mg OD, Tab Prednisolone 5mg BD. Injection of Leucoverin 1.5ml 6 hourly Intravenous over 1 mint was given. After patient blood grouping and cross-matching were done 6-pint random donor platelets and 1-pint packed cell volume transfusion was done.He was empirically started on broad-spectrum antibiotics for neutropenic fever and MTX was stopped. He improved significantly and pancytopenia resolved with almost normal hematology in a week of follow up and was discharged on day 7.
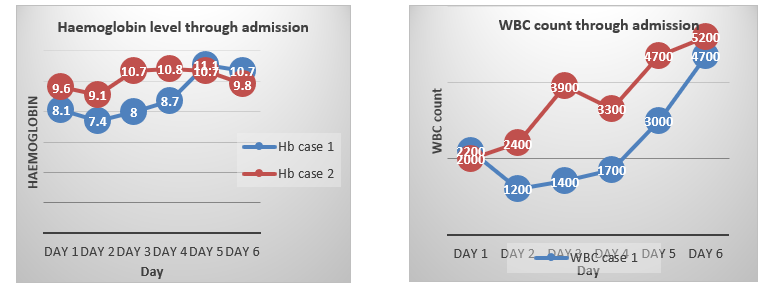
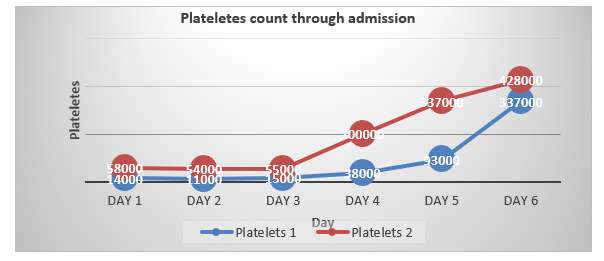
Table 1: Clinical and laboratory parameters.
|
Parameters |
Day 1 |
Day 2 |
Day 3 |
Day 4 |
Day 5 |
Day 6 |
|
Haemoglobin (g/dl) |
8.1 | 7.4 | 8.0 | 8.7 | 11.1 | 10.7 |
|
White blood cells(cu/mm) |
2200 |
1200 |
1400 |
1700 |
3000 |
4700 |
|
Platelets (mcl) |
14000 |
11000 |
15000 |
38000 |
93000 |
337000 |
Case Report 2
A 76 year male was admitted in the Bombay port trust hospital in a ward with a chief complaint of bleeding from the groin region associated with burning, itching, pain, foul smelling with skin maceration over the scrotum and penis, low back pain, severe generalized weakness, increased frequency of urination. On examination patients’ vitals were as P=116/min, BP= 140/90 mm hg, built= obese, Nutrition =good, Weight=97 kg, and pallor was present. No icterus/ cyanosis/ skin /clubbing, or Oedema/ JVP found. The patient was diagnosed with Frictional dermatitis in a known case of diabetes, hypertension, and psoriasis. The patient was on methotrexate for 1 year. Admitted similar complaints in past. Systemic examination was within normal limits. The patient was diagnosed with MTX-induced pancytopenia. On admission patient's blood glucose, was 327mg/dl, urea;51, creatinine; 1.3, alt(pt); 59, bilirubin; 0.4mg/dl while at the time of discharge blood glucose; 477mg/dl, urea;41, creatinine; 1.71, alt(pt); 40, bilirubin; 0.4mg/dl. Serum acetone was absent with no derangement of the lipid profile. Urine Routine /Microscopic e/o; Sugar ++, Hb ++++, RBC plenty, WBC 2-3 HPF, EC 1-2 hpf.
Treatment Given
Oral hypoglycemic drugs, anti-hypertensive drugs given. On skin lesion Liquid Paraffine, Soframycine Powder, and Mupirocin Ointment for local application were given twice a day on the groin region. For low back pain, diclofenac gel and an injection of tramadol in 100ml of Normal saline were given. Empirically antibiotic (injection Amoxcycillin+ clavulanic acid 1.25gm BD), anti-fungal (injection Flucanozole 100mg OD), antiemetic (ondansetron 4mg TDS), and antacid (pantoprazole 40mg OD) were added for 5 days. The patient's condition improved gradually within a week of treatment. The patient was withheld from tablet methotrexate during treatment.
Table 2: Clinical and laboratory parameters.
|
Parameters |
Day 1 |
Day 2 |
Day 3 |
Day 4 |
Day 5 |
Day 6 |
|
Haemoglobin (g/dl) |
9.6 | 9.1 | 10.7 | 10.8 | 10.7 | 9.8 |
|
White blood cells (cu/mm) |
2000 |
2400 |
3900 |
3300 |
4700 |
5200 |
|
Platelets (mcl) |
58000 |
54000 |
55000 |
200000 |
337000 |
428000 |
Discussion
Methotrexate (MTX) is a dihydrofolate reductase (DHFR) inhibitor. High-dose MTX (0.5 - 12 g/m2) has antiproliferative activity and is used in the treatment of cancer while low-dose MTX (10 - 40 mg/m2) has anti-inflammatory and immunosuppressive properties [1].
In the first case, the reported patient was taking a tablet of Methotrexate 5 Mg on Saturday, and Sunday and a tablet Folic Acid 5mg once a day Monday to Friday for 3 months. The patient did not have a proper outpatient monitor of CBC, creatinine, or liver function tests. Rheumatoid arthritis (RA) is a chronic autoimmune, systemic inflammatory disorder with characteristic deforming symmetrical polyarthritis of varying extent and severity. It is associated with synovitis of joint and tendon sheaths, articular cartilage degradation, erosion of juxta-articular bone, positive IgM rheumatoid factor, and anticitrullinated protein antibodies (ACPAs) [4]. On admission patient's Haemoglobin was 7.4 gm, WBC was 1200/cu mm, Platelets were 1100, serum creatinine was 1.53 mg/dl, and was diagnosed as MTX-induced pancytopenia. The patient was given leucovorin intravenously. On the day before discharge, her Haemoglobin was 9.8 gm, WBC 5200/cu mm, and Platelets were 428000.Her LFT and RFT were within normal limits showing no toxicity in the liver and kidney. A similar case report of pancytopenia was reported by Ibarra et.al in which the patient was advised methotrexate 7.5 mg weekly dose to 2.5 mg daily for approximately two months which leads to pancytopenia: WBC (2.0; differential: polys = 23%, lymphocytes = 55%, monocytes = 2%, and eosinophils = 20%), Hb (7), MCV (89), and platelets (3000). Her last CBC two months prior was WBC (7.6), Hb (10.2), and platelets (194) [5].
In the Second case, reported pancytopenia was associated with methotrexate which the patient was taking for psoriasis management, later he was diagnosed with frictional dermatitis [6]. In this case, patient HB was 9.6gm/dl, WBC;2000 cumm, platelets; 58000, random blood glucose;327mg/dl, Urea; 51mg/dl, sr. creatinine;1.3gm/dl. The patient was given anti-diabetic, anti-hypertensive, antifungal, and symptomatic management. Injection leucovorin was not used. On the 12th day of discharge, patient HB was 9.8 gm/dl, WBC;5200 cumm, platelets; 428000. The patient's general condition improved.Pankti Jariwala, et al also reported Similar two Cases of psoriasis that showed the side effect of MTX as pancytopenia, among them the first patient was a 50-year-old male of psoriasis on intermittent treatment with MTX. After a treatment-free period of six months, he had self-medication of MTX along with analgesic for joint pain for one week which followed ulceration of the lesions, bone marrow suppression, and eventually death. The second patient was a 37-year-old male with psoriasis, who has taken MTX one week earlier without prior investigations. He had painful ulcerated skin lesions and bone marrow suppression. On investigations, he showed a high creatinine level and a non-functioning right kidney on ultrasonography. Despite dialysis, he succumbed to death.[6]
Bone marrow toxicity, in most cases, is dose-dependent and responds to folic acid administration. Pancytopenia, leukopenia, anemia, and thrombocytopenia can occur but are rare. In a review by Gutierrez-Urena and associates, clinically significant pancytopenia was found in 1% to 2% of RA patients on MTX therapy. The mucocutaneous toxicities of MTX, which have been reported to occur in up to one-third of patients, are dose-dependent and respond to folate replacement [5][7].
Immediate discontinuation of MTX is of utmost importance. Supportive measures include leucovorin (folinic acid), alkalinization of urine, intravenous hydration, G-CSF, and blood products [2]. Other options include hemoperfusion and hemodialysis. Although corticosteroids are frequently administered, there are no large trials suggesting their efficacy yet and may increase the risk of superinfections due to coexisting neutropenia in our case. [10]
There should be proper counseling for the patient for not taking the drugs on their own without consulting a dermatologist as well as not to combine them with any other drug without taking doctors' consent. The newer therapeutic measures and alternative methods may be adopted in case of management of chronic and autoimmune diseases such as RA and Psoriasis which as widely used since ancient times with maximum effect and minimum side effects. This Unani system of medicine/ traditional Persian medicine and Ayurveda may be more effective and safer than conventional methotrexate. A randomized control trial of efficacy and safety for the treatment of chronic plaque psoriasis with herbal Unani formulations carried out by Faiza et.al suggested that trial formulations, Itr?fal Sh?htra and Marham ?ina may be superior to control drugs PUVAsol and petrolatum in terms of safety, efficacy, and tolerability in the treatment of chronic plaque psoriasis. Similarly, for RA there are many clinical trials done.Verma et al carried out a study on 68 participants showing that the drug Habb-e-Asgand is therapeutically effective in the treatment of Waja ‘al-mafasil (rheumatoid arthritis). The results of the study were evaluated on clinical, biochemical, and hematological parameters and showed that the drug was nontoxic and safe [9].
Conclusion
This case report highlights the importance of early follow-up and regular laboratory investigations of patients on methotrexate therapy.Pre-treatment investigations are a must if MTX is to be prescribed. Proper monitoring and strict avoidance of self-administration of MTX are mandatory. Coadministration of the drugs like NSAIDs should be judicious. Selling such drugs without a prescription should be banned. And newer therapeutics regimens and Unani and Ayurveda systems should be used for management of the autoimmune disease.
Financial support and conflict of interest
The author(s) declared no conflicts of interest concerning the research, authorship, and/or publication of this article. The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Saigal S, Singh RK, Poddar B (2012) Acute methotrexate toxicity presenting as multiorgan failure and acute pneumonitis: A rare case report. Indian J Crit Care Med 16: 225-227.
- Ann Young, Daniel Beriault, Benjamin Jung, Anna Nikonova, Dory Abosh, et al. (2019) DAMPAned Methotrexate: A Case Report and Review of the Management of Acute Methotrexate Toxicity. Canadian Journal of Kidney Health and Disease 6: 1-6.
- Yosra Bedoui, Xavier Guillot, Jimmy Sélambarom, Pascale Guiraud, Claude Giry, et al. (2019) Review Methotrexate an Old Drug with New Tricks. Int. J. Mol. Sci 20: 5023.
- Ansari Umme Ammara Maqbool Ahmad et al. (2021) Etiopathogenesis and management of Waja‘al-maf??il (Rheumatoid arthritis): An evidence-based comprehensive review. Int. J. Res. Ayurveda Pharm 12: 96-103.
- Fernando Gonzalez-Ibarra, Sahar Eivaz-Mohammadi, Shiri Surapaneni, Hazem Alsaadi, Amer K. Syed et al. (2014) Case Report Methotrexate Induced Pancytopenia. Case Reports in Rheumatology 1: 1-4.
- Pankti Jariwala, Vinay Kumar, Khyati Kothari, Sejal Thakkar, Dipak Dayabhai Umrigar et al. (2014) Case Report Acute Methotrexate Toxicity: A Fatal Condition in Two Cases of Psoriasis. Case Reports in Dermatological Medicine 3.
- S Gutierrez-Urena, J. F. Molina, C. O. Garcia et al. (1996) Pancytopenia secondary to MTX therapy in rheumatoid arthritis. Arthritis and Rheumatism 39: 272–276.
- Faiza Khatoon, Mohd Azahar, Arzeena Jabeen, Qamar Uddin, Nazim Husain et al. (2022) Treatment of chronic plaque psoriasis with herbal Unani formulations: A randomized control trial of efficacy and safety. Journal of Ethnopharmacology 296: 1154-1156.
- R S Verma, P Khan, S Ayub, S Afzal, J Akhtar et al. (2021) Efficacy and safety of an Unani compound drug– Habb-e-Asgand in Waja‘al-Mafasil (Rheumatoid Arthritis) cases- A preliminary study. Indian Journal of Traditional Knowledge 20: 8-14.