Inflammatory Myofibroblastic Tumor (IMT) of the Urinary Bladder: A Case Report
Rami Ghanem1*, Sohaib Alhamss2, Malek Gaashan1, Nour Alhisah1, Tayseer Afifi2
1Urologic Oncology & Robotic Surgery Consultant, Division of Urology, Department of Surgery, King Hussein Cancer Center, Amman, Jordan.
2Department of Surgery, Faculty of Medicine, Islamic University of Gaza, Palestine.
*Corresponding Author:Rami Ghanem, Urologic Oncology & Robotic Surgery Consultant, Division of Urology, Department of Surgery, King Hussein Cancer Center,P.O. Box 1269 Al-Jubeiha Amman 11941 Jordan, Tel: 00962795420286; Fax: 00962795420286; E-mail: ramighanem78@hotmail.com
Citation: Rami Ghanem, Sohaib Alhamss, Malek Gaashan, Nour Alhisah, Tayseer Afifi, et al. (2023)Inflammatory Myofibroblastic Tumor (IMT) of the Urinary Bladder-a Case Report. Cancer Prog Diagn 7: 134.
Received: February 24, 2023; Accepted: March 27, 2023; Published: March 30, 2023.
Abstract
Introduction
Since the discovery of Inflammatory myofibroblastic tumors (IMT) in 1980 by Roth, the etiology of this tumor remains poorly understood without a standardized treatment approach. It is a rare benign soft tissue tumor in the genitourinary tract so, it is also called pseudosarcomatous myofibroblastic proliferation. Management of IMT can be handled with minimally invasive bladder-sparing treatment.
Case Presentation
We report a case of a 26-year-old female with a four-month history of intermittent gross hematuria with the occasional presence of clotted blood within urine without dysuria or irritative lower urinary tract symptoms which is treated by partial cystectomy and followed up by cystoscopy without detection of local recurrence.
Conclusion
Early follow-up cystoscopy and radiological follow-up for 1 year are recommended for local recurrence detection.
Keywords
Inflammatory Myofibroblastic Tumor, Urinary Bladder, Partial Cystectomy, Bladder Cancer.
Introduction
Bladder inflammatory myofibroblastic tumors (IMT) are uncommon soft tissue tumors. It is characterized as a submucosal stroma-based proliferative lesion with low or uncertain malignant potential [1]. IMT has formerly been referred to as plasma cell granuloma, pseudomalignant spindle cell proliferation, inflammatory pseudotumor, and pseudosarcomatous myofibroblastic tumor [2]. Diversity in nomenclature led to misunderstandings and difficulties in developing a single, standard treatment for this organism.
Among genitourinary tumors, IMT is most prevalent in the bladder; yet it accounts for less than 1% of all bladder tumors [3]. Roth reported the first incidence of IMT affecting the bladder in 1980 [1]. Even though dysuria and pelvic discomfort may be present, the most frequent presenting symptom for IMT in the bladder is painless hematuria [4]. Treatment options include transurethral resection of bladder tumor (TURBT), partial cystectomy, and/or radical cystectomy, depending on the specifics of the case.
The patient we reported was hospitalized for intermittent gross hematuria with the sporadic presence of coagulated blood in the urine, without dysuria or irritative symptoms of the lower urinary tract. The patient recovered smoothly after partial cystectomy, with no recurrence detected on regular follow-up one year later.
Case Report
A 26-year-old woman presented to the urology clinic with a 4-month history of intermittent total painless gross hematuria and an occasional history of clot passage. Her history of obstructive lower urinary tract symptoms includes intermittency, poor stream, straining, and dysuria, in addition to an occasional history of dyspareunia. She had no previous history of surgical operations or urethral instrumentation. She denied any previous smoking history. System evaluation and physical examination were ordinary.
Initial examinations included urine microscopy, which revealed red blood cells (RBCs) in excess of 50 per high-power field. Other urine microscopy values have been within normal levels. Urine culture revealed no growth, and cytology of urine revealed no cancer cells. Other laboratory results were a hemoglobin level of 12.6 g/dl and a creatinine level of 0.6 mg/dl.
Imaging examinations using an ultrasound of the urinary tract (US) revealed an immobile lesion measuring 5.4 cm near the dome of the bladder, with signs of internal vascularity on Doppler Ultrasound.
In response, she was sent for a computed tomography scan with intravenous contrast, which revealed a polypoid urinary bladder mass lesion starting from the dome and bursting into the lumen, measuring around 4.0 cm x 5.0 cm in dimensions. The contact between the bladder mass and precervical fat seems uneven and the lesion is partly calcified (Figure 1,2).
Transurethral resection of the bladder tumor (TUR-BT) was then performed after a further cystourethroscopy revealed a single lesion at the bladder dome with regions of calcification.
Submucosal spindle cell growth was structured in a fascicular and storiform pattern on a myxoid backdrop with a mixed inflammatory cell infiltration constituted mostly of lymphocytes, plasma cells, and dispersed eosinophils, which is indicative of an IMT.
Figure 1&2: A Computed tomography scan with I.V contrast showed: a polypoid urinary bladder mass lesion measuring about 4.0 cm X 5 cm in diameters originating from the dome and bulging into the lumen.
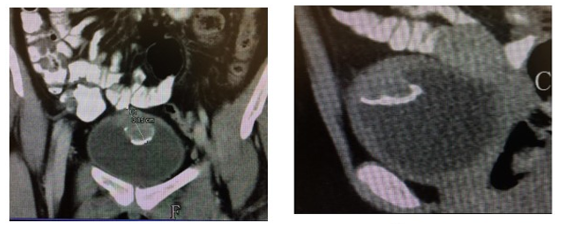
figugre(1) figure(2)
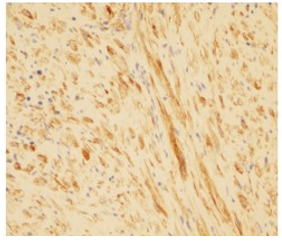
Additional immunohistochemical analysis revealed diffusely positive tumor cells for SMA (smooth muscle actin) (Figure3), ALK1, and P-catenin (cytoplasmic) (figure 4). Tumor cells do not express desmin, CD34, or C-kit.
A month after undergoing TURBT, the patient received a partial cystectomy through an extraperitoneal route with a 1 cm safety margin and a smooth postoperative recovery.
Figure 3: The spindle cells are positive for smooth muscle actin immunostaining (x20).
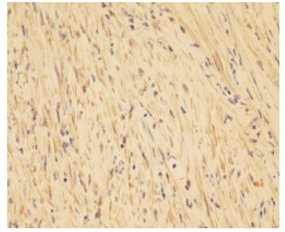
Figure 4: ALK-1 immunostaining is positive in tumor cells (x20).
The final pathology report indicated an IMT, totally removed with negative margins, regions of necrosis, and calcification, and no indication of urothelial neoplasia (shown in Figure 5, 6 ).
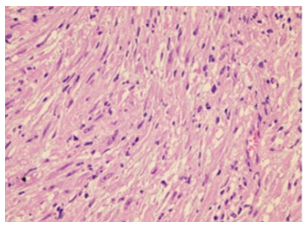
Figure 5: Low power view showing myofibroblastic spindle cells proliferation (H&E 10×).
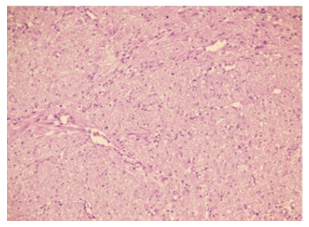
Figure 6: Closer view shows elongated myofibroblasts in a background of fibro-myxoid tissue abundant blood vessels and inflammatory cells. (H&E 20×).
Three and six months following the partial cystectomy, two check-up cystoscopies were done with no indication of recurrence.
Discussion
Teoh et colleagues evaluated 182 instances of IMT and observed a mean age of 38.9 years with a female predominance [5]. To the best of our knowledge, this case is one of the uncommon kinds of urinary bladder tumors. The precise etiology of IMT is unclear, however it has been linked to surgery, trauma, and infection; nonetheless, the vast majority of instances occur spontaneously.
IMTs of the urinary bladder resemble other aggressive spindle cell tumors such as rhabdomyosarcoma, making pathological identification difficult [6]. For accurate diagnosis and differentiation from other cancers, histological and immunochemical testing with the distinctive ALK marker is required.
IMTs are seen in several organs, including the lung, which is the most prevalent location, as well as the omentum, abdominal cavity, neck soft tissue, and retopertoneum [7]. Nonetheless, occurrence in the urinary bladder is uncommon.
In juvenile populations, the bladder dome is the most prevalent location of IMT, while in adult populations, the lateral bladder wall is the most common site.
An adult patient was discovered to have a pedunculated tumor emanating from the bladder dome. The patient presented with asymptomatic extensive hematuria with a protruding urethral lumb that causes dyspareunia and urinary obstruction.
Even if it is histologically benign, there is a possibility of sarcomatous potential, particularly pulmonary IMT with metastatic potential. Metastasis to the colon has been documented in just one instance of urinary bladder IMT after radical cystectomy. Local recurrence in the urinary bladder is often the result of an inadequate resection and not a real recurrence [8].
Ultrasound and computed tomography (CT) scans are the routine diagnostic procedures for assessing any bladder mass. However, transurethral resection and tissue analysis are necessary to confirm the diagnosis.
To prevent local recurrence, complete surgical resection is essential; nevertheless, medication has also been observed for non-resectable IMT. COX2 and VEGF were discovered in IMT and are suggested therapeutic targets. Pre-patient treatment with non-steroidal anti-inflammatory inhibitors (COX-2 inhibitors) to reduce tumor size prior to resection is recommended for both adult and pediatric patients with aggressive non-genitourinary IMT. Additionally, ALK inhibitor (Crizotinib) has been used in a few cases with a promising outcome. Regular imaging and cystoscopy are indicated for post-resection follow-up of local recurrence, however no precise procedure for follow-up has been established.
According to the majority of studies, the gold standard treatment for IMT in adults and children is complete transurethral resection of the lesion. Local recurrence has been reported in adults following incomplete surgical resection, but no proven recurrence or malignant episodes have been reported following surgical treatment [9].
Urinary bladder IMT is an uncommon, benign soft-tissue tumor that manifests with hematuria, dysuria, or urinary obstruction symptoms. Complete transurethral resection is the treatment of choice for IMT.
For the identification of local recurrence, early follow-up cystoscopy and radiological follow-up for one year are advised.
References
- Roth JA. (1980) Reactive pseudo sarcomatous response in urinary bladder. Urology 16: 635-637.
- Song D. (2019) Inflammatory myofibroblastic tumor of urinary bladder with severe hematuria: A Case report and literature review. Medicine 98(1).
- Montgomery EA, Shuster DD, Burkart AL, Esteban JM, Sgrignoli A et al. (2006) Inflammatory myofibroblastic tumors of the urinary tract: a clinicopathologic study of 46 cases, including a malignant example inflammatory fibrosarcoma and a subset associated with high-grade urothelial carcinoma. The American journal of surgical pathology 30: 1502-1512.
- Patnana M, Sevrukov AB, Elsayes KM, Viswanathan C, Lubner M et al. (2012) Inflammatory pseudotumor: the great mimicker. American Journal of Roentgenology 198: 217-227.
- Teoh JY, Chan NH, Cheung HY, Hou SS, Ng CF et al. (2014) Inflammatory myofibroblastic tumors of the urinary bladder: a systematic review. Urology 84: 503-508.
- Machioka K, Kitagawa Y, Izumi K, Kitamura S, Ikeda H et al. (2014) Inflammatory myofibroblastic tumor of the urinary bladder with benign pelvic lymph node enlargement: a case report. Case reports in oncology 7: 571-575.
- Coffin CM, Watterson J, Priest JR, Dehner LP et al. (1995) Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor) a clinicopathologic and immunohistochemical study of 84 cases. The American journal of surgical pathology 19: 859-872.
- Collin M, Charles A, Barker A, Khosa J, Samnakay N et al. (2015) Inflammatory myofibroblastic tumour of the bladder in children: a review. Journal of Pediatric Urology 11: 239-245.
- Houben CH. (2007) Pseudosarcomatous myofibroblastic proliferations of the bladder: a clinicopathologic study of 42 cases. The American journal of surgical pathology 31: 642.