Hungry and Stressed? Take A Mouthful of This Awful Delicacy
Sail DB1*, Babhulkar S1, Kadam K1, Thakur SS2, Umrajkar H2, Kulkarni PS2
1 Department of Psychiatry, B. J. medical college & Sassoon General Hospital, Pune, India.
2 Department of Surgery, B. J. medical college & Sassoon General Hospital, Pune, India.
*Corresponding Author:Sail DB, Department of Psychiatry, B. J. medical college & Sassoon General Hospital, Pune, India, Tel: 020 2612 8000; Fax: 020 2612 8000; E-mail: durvasail@gmail.com
Citation: Sail DB, Babhulkar S, Kadam K, Thakur SS, Umrajkar H, et al. (2022) Hungry and Stressed? Take A Mouthful of This Awful Delicacy. Archiv Neurol Neurosurgery 3: 122.
Received: November 07, 2022; Accepted: December 04, 2022; Published: December 07, 2022.
Copyright: © 2022 Sail DB, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Trichotillomania was first described by Hallopeau over 100 years ago which is characterized by repetitive rituals performed with hair after it has been removed, and has a prevalence of 0.6%– 1.6% [1]. Strong female predilection is noted with this disorder and typically affects patients in childhood and adolescence. Around 30% of patients who suffer from trichotillomania were also found to be engaging in trichophagia. Among these around 1%, require surgical intervention due to complications of the resulting trichobezoars, which are indigestible masses of hair lodged in the gastrointestinal tract [2]. But some studies have reported a 25%-37.5% prevalence of trichobezoar in those who engage in trichophagy [3,4]. Varying range of symptoms such as abdominal pain, chronic anorexia, failure to thrive, vomiting, and acute obstruction are seen as many trichobezoars go unnoticed. They may complicate resulting in mucosal erosion, ulceration, perforation, intussusception, obstructive jaundice, pancreatitis and even death have been reported in the literature [5]. If trichobezoar continue to grow and extend past the pylorus, this situation is called as Rapunzel syndrome was first described by Vaughan et al in 1968 [6].
Trichotillomania is often associated with young children and adolescents [7] with the average age of onset of trichotillomania is 12 years [4]. It is observed that trichotillomania develops in the background which is quite similar to the risk factors for child abuse. Various psychosocial stressors such as a disturbed mother-child relationship, parental separation or hospitalizations have been observed at the start of trichotillomania [8]. Hence psychiatric intervention becomes integral part of management to prevent recurrence [9]. We report a case of trichobezoar in 13 years old female referred for psychiatric assessment.
Case
A 13 years old female child referred to psychiatry department from surgery department in view of trichobezoar. On detailed evaluation, she reported that she experiencing anxiety features in the form of worrying thoughts & palpitations following stressor in the form of domestic violence & physical abuse at hostel. Following this she started experiencing persistent pervasive low mood, anhedonia, irritability, decreased appetite & easy fatigability for several months. In response to her anxiety she started plucking her hair & used to eat them to relieve it. During course of illness her school performance was also deteriorated. She lost weight as well. On physical examination Irregular, non-scarring, focal patches of alopecia, on the crown and left sided parietal region of the scalp was noted. Her BMI was 16.5 Kg/m2. Pallor was noted. On mental status examination her psychomotor activity was reduced with variable reaction time. She reported her mood as low and her affect was dysphoric. She was preoccupied with worrying thoughts and ideas of hopelessness, helplessness and worthlessness were noted. Diagnosis of Major Depressive Disorder with anxious distress as well as Trichotillomania was made as per DSM-5. On further investigation, her hemoglobin was 10 gm/dl and Barium meal, USG abdomen, CT abdomen patient were showing trichobezoar. Patient was operated for the same and started on Tab. Sertraline 25mg in view of depressive symptoms which was up titrated to 37.5 mg. She was enrolled in cognitive behavioral therapy. Parental counselling was done. Patient is maintained well on above treatment.
Figure 1: Irregular, non-scarring, focal patches of alopecia, on the crown

Figure 2: Surgical specimen of Trichobezoar.

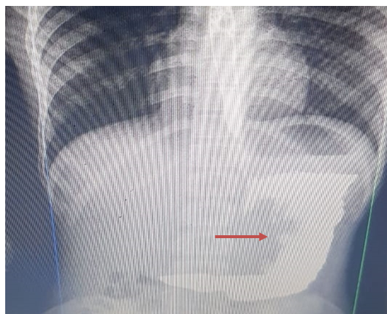
Figure 3: Barium meal showing a filling defect in stomach.
Discussion & Conclusion
As mentioned before, trichotillomania has female preponderance, usually starts in young children and adolescents [7], the average age of onset of trichotillomania being 12 years [4]. Irregular, non-scarring, focal patches of alopecia containing broken hair of varying length often on the crown, occipital, or parietal region on contralateral side to dominant hand are seen [10]. In a study 86% of women with trichotillomania reported a history of violence, suggesting a strong relationship of family chaos during childhood and trichotillomania [11]. Hence a child who presents with mechanical hair loss, may have either condition. Therefore, initial assessment should aim to confirm only the diagnosis of mechanical alopecia, keeping possibility of abuse in mind if hair pulling by the child is not witnessed [12] Studies on the pharmacotherapy of trichotillomania remain inconsistent, some stating patients seem to respond to fluoxetine or other serotonin reuptake inhibitors [13]. Parental counselling should also be a regular part of treatment to prevent recurrence [9]. The case exemplifies the need to keep a high index of suspicion not to miss child abuse. To recapitulate, one may consider that childhood depression with concomitant anxiety may present as trichotillomania, as an attempt to alleviate the mounting anxiety by hair pulling. So, attempt should be made to rule out co morbid depression in cases presenting as trichotillomania.
References
- O'Sullivan RL, Mansueto CS, Lerner EA, Miguel EC (2000) Characterization of trichotillomania: a phenomenological model with clinical relevance to obsessive-compulsive spectrum disorders. Psychiatric Clinics of North America 23: 587-604.
- Bouwer C, Stein DJ (1998) Trichobezoars in trichotillomania: case report and literature overview. Psychosomatic medicine 60: 658-60.
- Bhatia MS, Singhal PK, Rastogi V, Dhar NK, Nigam VR, et al. (1991) Clinical profile of trichotillomania. Journal of the Indian Medical Association. 89: 137-139.
- Cohen LJ, Stein DJ, Simeon D, Spadaccini E, Rosen J, et al. (1995) Clinical profile, comorbidity, and treatment history in 123 hair pullers: a survey study. The Journal of clinical psychiatry.
- Ahmad Z, Sharma A, Ahmed M, Vatti V (2016) Trichobezoar causing gastric perforation: a case report. Iranian journal of medical sciences 41: 67.
- Vaughan Jr ED (1968) The Rapunzel syndrome: an unusual complication of intestinal bezoar. Surgery 63: 339-343.
- Hallopeau M (1889) Alopecia par grattage (trochomanie or trichotillomania). Ann de Dermat et Syph. 10: 440-441.
- Oranje AP, Peereboom-Wynia JD, De Raeymaecker DM (1986) Trichotillomania in childhood. Journal of the American Academy of Dermatology. 15: 614-619.
- Cannalire G, Conti L, Celoni M, Grassi C, Cella A, et al. (2018) Rapunzel syndrome: an infrequent cause of severe iron deficiency anemia and abdominal pain presenting to the pediatric emergency department. BMC pediatrics. 18: 1-5.
- Mehregan AH (1970) Trichotillomania: a clinicopathologic study. Archives of Dermatology 102: 129-133.
- Smith RA, Ross JS, Bunker CB (1994) Localized trichorrhexis nodosa. Clinical and experimental dermatology 19: 441-442.
- Saraswat A (2005) Child abuse and trichotillomania. Bmj 330: 83-84.
- Swedo SE, Leonard HL, Rapoport JL, Lenane MC, Goldberger EL, et al. (1989) A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling). New England Journal of Medicine 321: 497-501.