Vaginal Microbiota Towards Cervical Intraepithelial Neoplasia (CIN) Screening Test. An Analytic Review
Chrisostomos Sofoudis 1*, Ludmila Baltaga 2, Spiros Delis 3
1 Department of Obstetrics and Gynecology, Konstantopoulio General Hospital, Athens, Greece.
2 Department of General Surgery ΙΙΙ, Westpfalz-Klinikum GmbH, Rheinland-Pfalz, Germany.
3 Department of General Surgery, Oncological Unit, Konstantopoulio General Hospital, Athens, Greece.
*Corresponding Author:Chrisostomos Sofoudis, Department of Obstetrics and Gynecology, Konstantopoulio General Hospital, Athens, Ippokratous 209, 11472, Athens, Greece, Tel: 00306943662013; Fax: 00306943662013
Citation: Chrisostomos Sofoudis, Ludmila Baltaga, Spiros Delis (2024) Vaginal Microbiota Towards Cervical Intraepithelial Neoplasia (CIN) Screening Test. An Analytic Review. Cancer Prog Diagn 8: 146.
Received: March 09, 2024; Accepted: April 10, 2024; Published: April 18, 2024.
Copyright: © 2024 Aurelian Udristioiu, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Running Title
Vaginal Microbiota Implication as Cervical Intraepithelial Neoplasia (CIN) Primary Screening Test
Abstract
Background: Vaginal microbiota has recently come to light as a new promising indicator of intraepithelial neoplasia. Bacterial dysbiosis appears to initiate a cytological pathway favorable to cancerous alterations. Therefore, the present systematic review was performed with the purpose of particularizing the microorganisms most often involved, the relevance with HPV infection, as well as microbiome’s impact on precancerous alterations.
Methods: Following assiduous research up to August 2022 of the Pubmed and Cochrane databases inserting the terms ‘vaginal microbiota AND dysplasia OR cervical intraepithelial neoplasia, a total of 10 articles were selected. Studies with clearly defined objectives and studied microorganisms were included. Exclusion criteria was a population number less than 20 people.
Results: An HPV infection bears a positive correlation with an abundance of Gartenella and Prevotella colonies and a negative one with Lactobacillus. Lactobacillus seems to have a protective role against HPV. Subsequently a Lactobacillus-depleted microbiota has proven to facilitate the progression of CIN severity.
Conclusion: Our findings suggest a strong bond between vaginal microbial population, predisposed for CIN development. Moreover, it presents a plethora of other clinical possibilities which favor the use of vaginal microbiota as a screening tool.
Keywords
Vaginal Microbiota; Cervical Intraepithelial Neoplasia (CIN), Human Papillomavirus (HPV); Lactobacillus Spp; Persistent Vaginal Infection; Carcinogenic Factors.
Introduction
Cervical dysplasia is characterized by the abnormal growth of cells on the surface of the cervix. This allows the entrance into the cervical tissue of human papillomavirus (HPV), which accounts for approximately 90% of cervical cancer cases. [1]
An estimated 500 000 people are diagnosed with cervical cancer yearly worldwide. Risk factors include HPV or herpes infection, immunodeficiency, smoking, age, oral contraceptives, socioeconomic factors, and exposure to diethylstilbestrol (DES). As far as age is concerned, the risk of developing cervical cancer peaks during the late teens and mid-30s and remains stable, requiring regular check-ups. [2]
HPV alone seems to be responsible for a high percentage of cases of cervical dysplasia. In Greece, the incidence of HPV infection is up to 50%, with the vaccination coverage remaining low up to the present date. [3]
Intestinal metaplasia affects the glandular epithelium of the endocervix. It is a metaplastic precursor of cervical cancer with the first case reported in 1965. Possible mechanisms are either a preexisting heteroplastic or metaplastic mucosa that precedes the development of neoplasia or metaplastic changes coinciding with the malignant transformation. [4]
Approximately 30 types of HPV are known to affect the genital tract, 15 of which are characterized as ‘high-risk’ and are associated with high-grade lesions and invasive cervical cancer. Of those, HPV16 and HPV18 cause the vast majority of squamous cell carcinomas and adenocarcinomas. Another 11 types, classified as ‘low-risk’, result in genital warts and benign cervical lesions. [Table 1] [5]
HPV alone is not likely to induce cancer, as genetic and epigenetic alterations are also required. Its mechanism of action results from the role of E6 and E7 oncogenic proteins in regulating the cell cycle, specifically apoptosis. The disruption of E2 protein’s mechanism follows, which normally suppresses the E6 and E7. Lastly, immune evasion is promoted through the expression of the E5 oncogene. A combination of the above-mentioned pathways results in carcinogenesis. [6]
The two main types of dysplasia are Low-grade Squamous Intraepithelial lesion (LSIL) and High-grade Squamous Intraepithelial Lesion (HSIL), which are potential precancerous states. [Figure 1] [Table 2] [7]
Figure 1: Cervical infiltration staging.
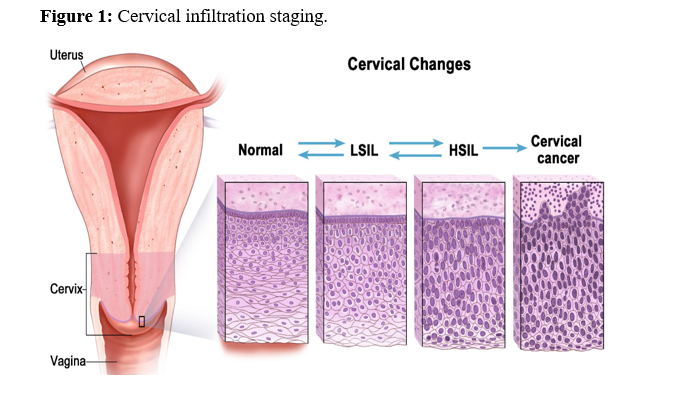
Table 1: Clinical depiction of HPV infiltration.
|
Disease |
HPV type |
|
Plantar warts |
1, 2, 4, 63 |
|
Common warts |
2, 1, 7, 4, 26, 27, 29, 41, 57, 65, 77, 1, 3, 4, 10, 28 |
|
Flat warts |
3, 10, 26, 27, 28, 38, 41, 49, 75, 76 |
|
Other cutaneous lesions (e.g., epidermoid cysts, laryngeal carcinoma) |
6, 11, 16, 30, 33, 36, 37, 38, 41, 48, 60, 72, 73 |
|
Epidermodysplasia verruciformis |
2, 3, 10, 5, 8, 9, 12, 14, 15, 17, 19, 20, 21, 22, 23, 24, 25, 36, 37, 38, 47, 50 |
|
Recurrent respiratory papillomatosis |
6, 11 |
|
Focal epithelial hyperplasia of Heck |
13, 32 |
|
Conjunctival papillomas/carcinomas |
6, 11, 16 |
|
Condyloma acuminata (genital warts) |
6, 11, 30, 42, 43, 45, 51, 54, 55, 70 |
|
Cervical intraepithelial neoplasia
Unspecified Low risk High risk |
30, 34, 39, 40, 53, 57, 59, 61, 62, 64, 66, 67, 68, 69 6, 11, 16, 18, 31, 33, 35, 42, 43, 44, 45, 51, 52, 74 16, 18, 6, 11, 31, 34, 33, 35, 39, 42, 44, 45, 51, 52, 56, 58, 66 |
|
Cervical carcinoma |
16, 18, 31, 45, 33, 35, 39, 51, 52, 56, 58, 66, 68, 70 |
The grade of dysplasia is determined by the percentage of dysplastic cells in the cervical epithelium. Thus, the lower ? or less of the epithelium corresponds to low-grade or Cervical Intraepithelial Neoplasia (CIN) 1, while the invasion of the 2/3 of the epithelium corresponds to high-grade or CIN-2 and in situ to CIN-3. As the basement membrane is going to be penetrated, dysplasia depicts malignant infiltration. [8]
The primary screening method includes a Pap smear, colposcopy and potential cervical biopsy. The newest screening guidelines introduce the idea of cervical cancer testing to all patients with a cervix aged from 25 to 65, with either an HPV test done every 5 years, a combination of HPV and Papanicolaou smear testing every 5 years, or a Pap test alone every 3 years. [9]Routine vaccination against HPV is recommended for both sexes at the age of 11 or 12 years and includes two doses given 6 to 12 months apart. Vaccination after the age of 26 is not normally recommended, with the final decision based on a thorough discussion with a clinician.
Three types of vaccines are currently available. The bivalent Cervix is given in two doses six months apart for people aged 9 to 14 years and in three doses for people aged 15 and above. The quadrivalent Gardasil is administered in three doses at 0, 2 and 6 months. Lastly, the 9-valent Gardasil is given to patients from 9 through 14 years in either two or three doses apart, starting at 0, 6, 12 or 1, 2, 6 months respectively. Patients from 15 through 45 years receive a regimen of three doses and intervals of 0, 2 and 6 months. [10]
Table 2: Cervical infiltration cytological and histological classification.
|
Cytological classification (used for screening) |
Histological classification (used for diagnosis) |
||
|
Pap-test |
Bethesda System |
CIN |
WHO |
|
Class I |
Normal |
Normal |
Normal |
|
Class II |
ASCUS ASC-H |
Atypia |
Atypia |
|
Class III |
LSIL |
CIN1 including flat condyloma |
Koilocytosis |
|
|
HSIL |
CIN2 |
Moderate dysplasia |
|
|
HSIL |
CIN3 |
Severe dysplasia |
|
Class IV |
HSIL |
CIN3 |
Carcinoma in situ |
|
Class V |
Invasive carcinoma |
Invasive carcinoma |
Invasive carcinoma |
ASCUS: atypical squamous cell of undetermined significance, ASC-H: atypical squamous cells, cannot exclude a high-grade squamous intraepithelial lesion, CIN: cervical intraepithelial neoplasia, LSIL: low-grade squamous intraepithelial lesion, HSIL: high-grade squamous intraepithelial lesion.
The vaginal microbiota is composed of a plethora of microorganisms, of which Lactobacillus crispatus, L. jensenii, and L. gasseri are the main ones and commonly cohabit in an equilibrium. [Table 3]
Table 3: Vaginal microbiota classification.
|
Gram-positive aerotolerant anaerobes cocci and bacilli |
Lactobacillus Streptococcus |
|
Gram-positive facultative anaerobes cocci and bacilli |
Corynebacterium Gartenella Staphylococcus (mainly S.epidermidis) |
|
Gram-negative facultative anaerobes bacilli |
Escherichia Klebsiella Proteus |
|
Micoplasmas |
Mycoplasma (especially M.hominis) Ureaplasma |
|
Gram-positive strict anaerobes cocci and bacilli |
Atopobium Peptococcus Peptostreptococcus Clostridium Bifidobacterium Propionibacterium Eubacterium |
|
Gram-negative strict anaerobes bacilli |
Bacteroides Prevotella |
Their role is to protect the vaginal mucosa from harmful pathogens by producing antimicrobial substances, and co-aggregation with the pathogens thus eliciting a microbicidal effect as well as blocking the colonization of the vaginal epithelium by pathogens. [11]
In women of reproductive age, the pH of the lower vagina estimated around 4.5, a value determined by the lactic acid produced by Lactobacillus spp. that dominates the healthy vaginal microbiome. [12]
Aging, particularly after the age of 45, has proved to lead to an increase in vaginal pH, with menopause being another factor diminishing cervical acidity. [13]
Fluctuation in cervical microbiota’s composition is induced mainly by the menstrual cycle status and sexual activity, with other still unknown factors certainly playing a role. [14]
Material and Methods
Search Strategy
An assiduous analysis was performed throughout Pubmed and Cochrane databases until September 2022, entering the term ‘vaginal microbiota’ and selecting clinical trials and randomized controlled trials. The following search was restricted to the last decade and the language to English. A total of 10 articles were selected (Table 4), based on the following inclusion criteria: (1) patients with no previous surgical intervention in the uterine cavity, (2) known HPV infection, (3) sexually active patients. Exclusion criteria reflect previous hysterectomy, sexual intercourse or douching the previous 48h prior to the sample taking, history of cervical or other lower genital cancer as well as destructive therapy of the cervix.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism 9 Software. All statistical values were reported with 95% Confidence Intervals (CI), whereas statistically significant was interpreted as a p-value less than 0.05. Further subgroup analyses were focused on parameters such as the positive and negative impact of an HPV infection and a CIN progression on the vaginal microbiota.
Study Selection and Characteristics
The selected studies refer to a time frame between 2015 and 2022, with a population ranging from a minimum of 69 up to 448 women. Mean age was calculated at about 34.2 years. From the studied women, about 15.53% were current or past smokers with a history of more than 100 lifetime cigarettes and 45.28% used any of the following contraceptive methods: pill, injectable, condom.
Table 4: Study group’s demographic characteristics.
|
Author |
Year |
Population nr. |
Age (years) |
Smoker n(%) |
Contraceptive use n(%) |
HPV without CINs n(%) or Normal group |
LSIL n(%) |
HSIL n(%) |
ICC n(%) |
|
Mitra et al. [27] |
2015 |
169 |
31 |
41 (24.26) |
63 (37.28) |
20 (11.83) |
52 (30.77) |
92 (54.44) |
5 (2.96) |
|
Dareng et al. [28] |
2016 |
278 |
36.05 |
8 (2.88) |
62 (22.3) |
NS |
NS |
NS |
NS |
|
van de Wijgert et al. [29] |
2019 |
448 |
34 |
50 (11.16) |
113 (25.2) |
NS |
NS |
NS |
NS |
|
Usyk et al. [30] |
2020 |
273 |
22.9 |
65 (23.8) |
263 (96.33) |
NS |
NS |
NS |
NS |
|
Chen et al. [31] |
2020 |
229 |
45.26 |
NS |
NS |
78 (34.01) |
51 (4.87) |
23 (10.04) |
9 (3.93) |
|
Wu et al. [32] |
2020 |
69 |
38.5 |
NS |
NS |
31 (44.93) |
22 (31.88) |
16 (23.19) |
0 (0) |
|
McKee et al. [33] |
2020 |
109 |
26 |
NS |
NS |
55 (50.46) |
45 (37.19) |
6 (4.96) |
3 (2.48) |
|
Zhai et al. [34] |
2021 |
168 |
41.19 |
NS |
NS |
58 (34.52) |
32 (19.05) |
40 (23.81) |
38 (22.62) |
|
Carter et al. [35] |
2021 |
84 |
29 |
NS |
NS |
NS |
NS |
NS |
NS |
|
Lin et al. [36] |
2022 |
448 |
38.05 |
NS |
NS |
NS |
NS |
NS |
NS |
CIN intraepithelial neoplasia, LSIL Low-grade squamous intraepithelial lesions, HSIL High-grade squamous intraepithelial lesions, ICC Invasive cervical cancer, NS not specified.
Results
HPV or possible precancerous lesions were not specified in five studies. The resulting data portrayed a total of 35.15% women either healthy or presenting an HPV infection without CIN, 24.75% women with low-grade squamous intraepithelial lesions, 23.89% with a high-grade squamous intraepithelial lesion and 6.4% women with invasive cervical cancer.
Lactobacillus and Gardnerella vaginalis are the most abundant microorganisms found in a healthy vagina. An HPV infection seems to increase Gardnerella and Prevotella abundance, while diminishing the number of Lactobacillus population. No statistically significant result could predict an association in the progression of CIN severity. [Table 5].
Discussion
We performed an analytic review of the current bibliography pertaining to the vaginal microbiota as a possible biomarker of intraepithelial neoplasia. Though a correlation between the type of prevailing vaginocervical micro-organisms and the development of precancerous lesions has been widely speculated, the up-to-date literature has not yet brought to light substantial evidence.
Our study deduces Lactobacillus as the most abundant vaginal microorganism, whose population significantly diminishes with an HPV infection. Similarly, Gartenella and Prevotella abundance is positively correlated with an HPV condition. Moreover, a Lactobacillus-depleted microbiota has proven to facilitate the progression of CIN severity.
Table 5: Vagina’s microbial population.
|
Author |
Year |
Most abundant microorganism |
Positive HPV impact on its abundance |
Negative HPV impact on its abundance |
Positive association with the progression of CIN severity |
Negative association with the progression of CIN severity |
|
Mitra et al. [27] |
2015 |
Lactobacillus spp.
|
NS
|
Lactobacillus crispatus, Lactobacillus jensenii
|
Lactobacillus-depleted, Sneathia sanguinegens, Anaerococcus tetradius, Peptostreptococcus anaerobius
|
Lactobacillus spp, Lactobacillus crispatus |
|
Dareng et al. [28] |
2016 |
Prevotella, Leptotrichia
|
Lactobacillus sp., L. crispatus, L. iners
|
NS |
NS |
|
|
van de Wijgert et al. [29] |
2019 |
Lactobacillus iners |
NS |
Lactobacillus crispatus or jensenii |
NS |
NS |
|
Usyk et al. [30] |
2020 |
Lactobacillus, Gardnerella vaginalis |
NS |
NS |
||
|
Chen et al. [31] |
2020 |
Lactobacillus, Firmicutes, Actinobacteria, Bacteroidetes, Fuso- bacteria, Proteobacteria |
Prevotella, Bacillus, Anaerococcus, Sneathia, Megasphaera, Streptococcus and Anaerococcus, Bacteroidetes, Sneathia sanguinegens, Bifidobacterium unclassified, Candidatus Mycoplasma, Comamonadaceae, Veillonella montpellierensis, Faecalibacterium, Finegoldia unclassified, Fusobacterium mortiferum, Porphyromonas uenonis, Ralstonia pickettii, Fusobacteria, Proteobacteria, Sneathia sanguinegens, Bifidobacterium unclassified, Candidatus Mycoplasma, Comamonadaceae, Veillonella montpellierensis, Faecalibacterium, Finegoldia, Fusobacterium mortiferum, Porphyromonas uenonis, Ralstonia pickettii |
Lactobacillus, Gardnerella, Atopobium |
Bacillus, Anaerococcus |
Gradnerella vaginalis |
|
Wu et al. [32] |
2020 |
Lactobacillus |
NS |
NS |
NS |
Peptostreptococcaceae, Pseudomonadales |
|
McKee et al. [33] |
2020 |
Gardnerella vaginalis, L. iners, L. crispatus |
Gardnerella vaginalis |
Lactobacillus spp., L. iners, L. gasseri. |
|
|
|
Zhai et al. [34] |
2021 |
Lactobacillus (Firmicutes), Gardnerella (Actinobacteria) |
Gardnerella, Prevotella |
Lactobacillus, Ignatzschineria |
Gardnerella and Prevotella |
Lactobacillus, Ignatzschineria |
|
Carter et al. [35] |
2021 |
NS |
Lactobacillus crispatus |
NS |
NS |
|
|
Lin et al. [36] |
2022 |
Lactobacillus, Firmicutes |
Gardnerella, Prevotella, Actinobacteria, Bacteroides |
Firmicutes |
NS |
NS |
These findings support the idea of further development of existing vaginal microbiome screening tests, which offer promising diagnostic and therapeutic possibilities. Thus, vaginal microbiota componency could be used as a biomarker in screening the general population for CIN or its predisposure. [15]
Further possibilities would be suppressing certain pathogen microorganisms that favor precancerous lesions but also further infections, such as bacterial vaginosis and other relevant infectious entities. [16]
A special focus could be placed on vaginal microbiome transplantations as a possible preventive or therapeutic method against CIN lesions. [17]
Microbial dysbiosis is associated with unfavorable obstetric outcomes and complications. Specifically, it increases the risk of spontaneous preterm birth. Early vaginal cultures have been suggested as a predictor factor of a pregnancy’s outcome. A microbiota-based diagnosis and therapy is therefore encouraged for further studies. [18]
Furthermore, we propose that the association between vaginal microbiota and reproductive health, particularly infertility among women, should be analyzed extensively. Hong, X. et al. suggests a negative correlation between a Lactobacillus rich vaginal microbiota and female infertility. [19]
Skafte-Holm et al. indicates a negative impact of vaginal dysbiosis on pregnancy rates per embryo transfer in in vitro fertilization (IVF). [20]
The vaginal microbiota could be also studied as a tool to predict IVF success. Koedooder et al. suggests a division into favorable and unfavorable microbiome profiles of the vaginal microbiota, with specific characteristic and microbial populations of each. [21]
As estrogen is regulated by the gut microbiota through secretion of β-glucuronidase, it subsequently impacts the vaginal microbiome. Thus, it safe to admit that further studies of the gut microbiome would have a strong impact on understanding and modulating the vaginal microbiota. [22]
Limitations
The current study has several limitations. The scarceness of up-to-date evidenced-based literature could potentially lead to biased results. Parameters such as onset of sexual activity, number of sexual partners, HPV vaccination, safe sexual practices and genetics influence the outcome. Thus, we propose further studies of vaginal microbiota focusing on detailed characteristics of the studies arms and their more accurate comparison.
Disclosure of Interest
All authors declare any financial interest with respect to this manuscript.
Conclusion and Take-away message
Vaginal microbiota seems to be the cornerstone for future studies of the female reproductive tract. As opposed to the uterine microbiota, its sample extraction is non-invasive, cheaper, less time-consuming and with significantly less discomfort for the patient. Its connection to the diagnosis and therapy of infections, cancerous lesions, as well as fertility and pregnancy outcome, sets a promising tone for the contemporary researcher and clinician.
It consists without doubt a significant role towards potential screening test of CIN (cervical intraepithelial neoplasia), especially in reproductive ages. Multidisciplinary approach seems mandatory, in order to establish proper diagnosis and therapeutic mapping.
References
- References
- Cooper DB, McCathran CE (2022) Cervical Dysplasia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–.
- Devarapalli P, Labani S, Nagarjuna N, Panchal P, Asthana S, et al. (2018) Barriers affecting uptake of cervical cancer screening in low- and middle-income countries: A systematic review. Indian J Cancer.
- Karamanidou C, Dimopoulos K, (2016) Greek health professionals’ perceptions of the HPV vaccine, state policy recommendations and their own role with regards to communication of relevant health information. BMC Public Health 16: 467.
- Azzopardi JG, Hou LT (1965) Intestinal metaplasia with argentaffin cells in cervical adenocarcinoma. J Pathol Bacteriol 90 :686-90.
- Gupta SM, Mania-Pramanik J (2019) Molecular mechanisms in progression of HPV-associated cervical carcinogenesis. J Biomed Sci 26: 28.
- Wang X, Huang X, Zhang Y (2018) Involvement of Human Papillomaviruses in Cervical Cancer. Front Microbiol 9: 2896.
- Darragh TM, Colgan TJ, Cox JT, Heller DS, Henry MR, et al. (2012) Members of LAST Project Work Groups. The Lower Anogenital Squamous Terminology Standardization Project for HPV-Associated Lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Arch Pathol Lab Med 136: 1266-1297.
- Cooper DB, McCathran CE. Cervical Dysplasia (2022) Jul 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–.
- 9.https://www.cancer.org/cancer/cervical-cancer/detection-diagnosis-staging/cervical-cancer-screeningguidelines.html
- https://www.cdc.gov/vaccines/vpd/hpv/hcp/recommendations.html
- Wang, Shuai (2017) “Antimicrobial Compounds Produced by Vaginal Lactobacillus crispatusAre Able to Strongly Inhibit Candida albicans Growth, Hyphal Formation and Regulate Virulence-related Gene Expressions.” Frontiers in microbiology 8: 564.
- Lykke MR, Becher N, Haahr T, Boedtkjer E, Jensen JS, et al. (2021) Vaginal, Cervical and Uterine pH in Women with Normal and Abnormal Vaginal Microbiota. Pathogens 10: 90.
- García-Closas M, Herrero R, Bratti C, Hildesheim A, Sherman ME, et al. (1999) Epidemiologic determinants of vaginal pH. Am J Obstet Gynecol 180:1060-1066.
- Gajer P, Brotman RM, Bai G, Sakamoto J, Schütte UM, et al. (2012) Temporal dynamics of the human vaginal microbiota. Sci Transl Med 4:132ra52.
- Lin S, Zhang B, Lin Y, Lin Y, Zuo X, et al. (2022) Dysbiosis of Cervical and Vaginal Microbiota Associated with Cervical Intraepithelial Neoplasia. Front. Cell. Infect. Microbiol 12:767693.
- Ling Z, Kong J, Liu F (2010) Molecular analysis of the diversity of vaginal microbiota associated with bacterial vaginosis. BMC Genomics 11: 488.
- Lev-Sagie A, Goldman-Wohl D, Cohen Y (2019) Vaginal microbiome transplantation in women with intractable bacterial vaginosis. Nat Med 25: 1500–1504.
- Di Simone N, Santamaria Ortiz A, Specchia M, Tersigni C, Villa P, et al. (2020) Recent Insights on the Maternal Microbiota: Impact on Pregnancy Outcomes. Front Immunol 11: 528202.
- Hong X, Ma J, Yin J, Fang S, Geng J, et al. (2020). The association between vaginal microbiota and female infertility: a systematic review and meta-analysis. Archives of Gynecology and Obstetrics.
- Skafte-Holm A, Humaidan P, Bernabeu A, Lledo B, Jensen JS, Haahr T. (2021) The Association between Vaginal Dysbiosis and Reproductive Outcomes in Sub-Fertile Women Undergoing IVF-Treatment: A Systematic PRISMA Review and Meta-Analysis. Pathogens 10: 295.
- Koedooder R, Singer M, Schoenmakers S, Savelkoul PHM, Morré SA, et al. (2019) The vaginal microbiome as a predictor for outcome of in vitro fertilization with or without intracytoplasmic sperm injection: a prospective study. Hum Reprod 34: 1042-1054.
- Baker JM, Al-Nakkash L, Herbst-Kralovetz MM (2017) Estrogen-gut microbiome axis: Physiological and clinical implications. Maturitas 103: 45-53.
- https://www.cancer.gov/publications/dictionaries/cancer-terms/def/cervical-dysplasia
- Burd EM (2003) Human papillomavirus and cervical cancer. Clin Microbiol Rev 16:1-17.
- Comprehensive Cervical Cancer Control: A Guide to Essential Practice. 2nd ed. Geneva: World Health Organization 2014.
- Martín R, Soberón N, Vázquez F, Suárez JE (2008) [Vaginal microbiota: composition, protective role, associated pathologies, and therapeutic perspectives]. Enfermedades Infecciosas y Microbiologia Clinica 26:160-167.
- Mitra A, MacIntyre D, Lee Y et al. (2015) Cervical intraepithelial neoplasia disease progression is associated with increased vaginal microbiome diversity. Sci Rep 16865.
- Dareng EO, Ma B, Famooto AO, Adebamowo SN, Offiong RA, et al. (2016) Prevalent high-risk HPV infection and vaginal microbiota in Nigerian women. Epidemiol Infect 144: 123-137.
- van de Wijgert JHHM, Gill AC, Chikandiwa A, Verwijs MC, Kelly HA, et al. (2020) HARP Study Group. Human papillomavirus infection and cervical dysplasia in HIV-positive women: potential role of the vaginal microbiota. AIDS 34:115-125.
- Usyk M, Zolnik CP, Castle PE, Porras C, Herrero R, et al. (2020) Costa Rica HPV Vaccine Trial (CVT) Group. Cervicovaginal microbiome and natural history of HPV in a longitudinal study. PLoS Pathog 16: e1008376.
- Chen Y, Qiu X, Wang W, Li D, Wu A, et al. (2020) Human papillomavirus infection and cervical intraepithelial neoplasia progression are associated with increased vaginal microbiome diversity in a Chinese cohort. BMC Infect Dis 20: 629.
- Wu M, Gao J, Wu Y, Li Y, Chen Y, et al. (2020) Characterization of vaginal microbiota in Chinese women with cervical squamous intraepithelial neoplasia. Int J Gynecol Cancer 30: 1500-1504.
- McKee KS, Carter KA, Bassis C, Young VB, Reed B, et al. (2020) The vaginal microbiota, high-risk human papillomavirus infection, and cervical cytology: results from a population-based study. Gynecol Pelvic Med 3:18.
- Zhai Q, Zhang W, Zhang Z, Fu Y, Li Y, et al. (2021) Characteristics of the Cervicovaginal Microenvironment in Childbearing-Age Women with Different Degrees of Cervical Lesions and HR-HPV Positivity. Pol J Microbiol 70: 489-500.
- Carter KA, Srinivasan S, Fiedler TL, Anzala O, Kimani J, et al. (2021) Vaginal Bacteria and Risk of Incident and Persistent Infection with High-Risk Subtypes of Human Papillomavirus: A Cohort Study Among Kenyan Women. Sex Transm Dis 48: 499-507.
- Lin W, Zhang Q, Chen Y, Dong B, Xue H, et al. (2022) Changes of the vaginal microbiota in HPV infection and cervical intraepithelial neoplasia: a cross-sectional analysis. Sci Rep 12: 2812.