Modern Military Neurotrauma and Its Complications in War Conditions in Megalopolis.
Lystratenko OI1*, Kardash AM2, Lystratenko DO3
1 Dr med in DoKTMO, Neurosurgical clinic. Donetsk.
2 Professor, Dr.med., Donetsk National Medical University, DoKTMO, Donetsk.
3 Intern in Neurosurgical clinic.
*Corresponding Author: Lystratenko OI, Dr med in DoKTMO, Neurosurgical clinic. Donetsk, TEL: +380503470088 ; FAX: +380503470088;E-mail:bezara22@gmail.com
Citation: Lystratenko OI, Kardash AM, Lystratenko DO (2019) Modern Military Neurotrauma and Its Complications in War Conditions in Megalopolis. Archiv Neurol Neurosurgery 3:111.
Copyright: : © 2019 Lystratenko OI, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received date: January 03, 2019; Accepted date: January 25, 2019; Published date: January 29, 2019.
Abstract
This work contains information about military neurosurgical traumas with their complications. Here will be spoken about neurosurgical medical treatment in the present military actions (local military conflict in Donbass from 2014 till nowadays). You can realize what kind of neurosurgical treatment could be used in megapolis which appears under fire. Content of the work: soft tissue- damages, open not penetrating wounds, open penetrating wounds with- and without- brain perforation. In addition will be noticed the difference between projectile (shrapnel) wounds and bullet wounds with their following treatment based on numerous cases of such kind of injuries. This work has some pictures in order to show pre- and post- operative patient’s condition.
Keywords
Battle trauma, war in megapolis, the organization of neurosurgical care, treatment, surgical rehabilitation.
Materials and Methods
Over the period from May 2014 to the present in the neurosurgery clinic more than 4000 people with closed and open (penetrating) head injuries (which were received during the military actions) was given appropriate neurocurgical care. Patients were examined with CT, MRI, radiography of the skull bones.
The patients were examined by traumatologists, ENT spetialists, oculists, maxillofacial surgeons, combustiologists, neuroreanimatologists. Time from injury to operation is up to 2 hours. The military actions are taking place in a megapolis (in a city with a population of 1 million inhabitants). The distance from the closest flashpoint till the neurosurgical clinic is approximately 13 km. The patients underwent neurosurgical operations - primary surgical treatment (PST) of gunshot wounds of the skull with the removal of hematomas, bone fragments and shell fragments, plastic of bone defects, skull surfaces.
Results
Wounds of soft tissues of the skull are up to 2000 people. Non-penetrating wounds of the skull bones are up to 1200 people. Penetrating craniocerebral injuries are up to 800 people.
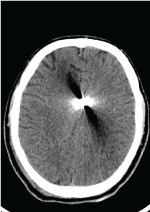
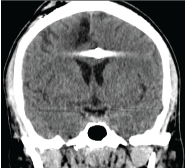
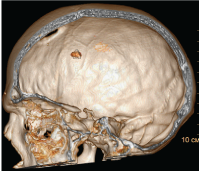
I group of patients is the most numerous. PST was provided in the next few hours from the moment of injury. Patients with concussion of brain were treated in the clinic of neurosurgery for a short time - up to 10 days [1]. The prognosis for life is favorable. For example – Figure: 1-3.

Figure 1

Figure 2

Figure 3
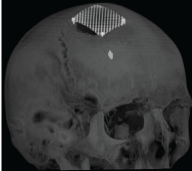
II Patient group - Characterized by a more severe course of head injury. Operations were carried out to remove bone fragments and shell fragments. Extensive skin defects were replaced with autografts. The plastic of extensive skin defects was carried out together with the combustiologists, as an urgent operation to prevent pyoinflammatory complications of the central nervous system [2]. Duration of stay of patients is up to 2 months, including several stages - such patients underwent reconstructive operations. The prognosis for life is favorable. Example – Figure: 4-8.

Figure 4: Reconstructive operation with implantation of endoexpander.

Figure 5

Figure 6

Figure 7
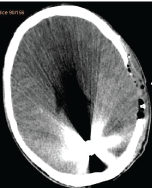
III The group of patients. The most severe category of patients is the group of patients with severe brain damage. Lethal outcome is up to 15% high degree of disability [3]. As a result - a long period of rehabilitation and social adaptation - up to 8 months. Bullet open penetrating wound of brain – Figure: 9-17. Projectile open penetrating wound of brain – Figure: 18-22.

Figure 9: Bullet stoped near C1.
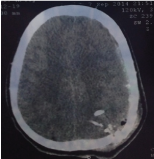
Figure 10

Figure 11
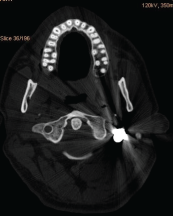
Figure 12
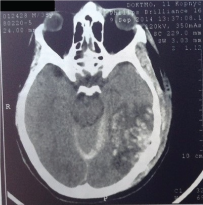
Figure 13: Postoperative photos.
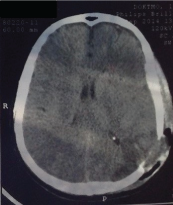
Figure 14
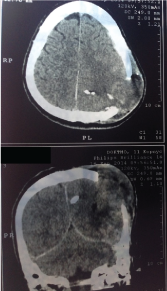
Figure 15: Fungus
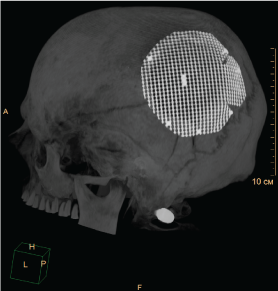
Figure 16: Plastic of defect after 7 month


This is a patient with an open penetrating projectile wound of the skull with a huge brain affection in occipital, left temporal regions. The patient was operated on. But prognosis is unfavorable due to huge brain affection with a lot of projectiles. Figure 23-25.
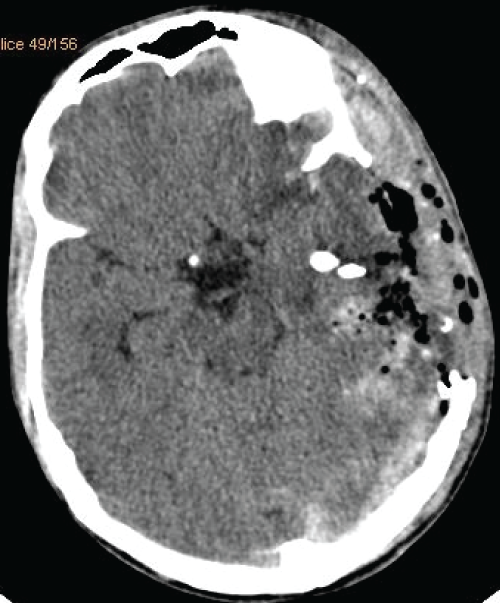
Figure 23
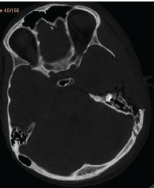
Figure 24
Conclusions
By modern military actions in a megalopolis conditions more than 50% of the injured are injured in the head. In military operations in addition to soldiers among the victims are a large number of civilians - up to 25%. During military actions in the megalopolis, the first medical aid was provided by ambulance teams, which delivered patients to the clinic of neurosurgery. The military first medical aid was given on the battlefield [4]. These patients were delivered by passing transport. Time from getting the wound to providing specialized neurosurgical care to all patients is up to 2 hours [5,6]. In connection with this the number of pyoinflammatory complications after treatment of patients with gunshot wounds to the skull is relative small - up to 1%. Died patients were in up to 20% of cases had combined wounds of the limbs, chest, abdomen, head.
So we determined that:
• The average time from admission of a patient till getting professional neurosurgical care should be not more than 2 hours.
• The number of pyoinflammatory infections by projectile wounds of the skull directly depend on the speed of receiving professional neurosurgical treatment.
• The projectiles with depth localization are not recommended to remove.
• Prognosis of life of patient damaged with projectile is higher, in comparison with damaged with bullet because of low kinetic force of projectile.
• By bullet wounds are taking place more tissue damages due-to higher kinetic force of bullet.
• Primary surgical treatment (PST) is performed outside the specialized center only because of vital indications to non-transportable patients. Transportable patients should be transported as quicker as possible in a specialized neurosurgical center in order to reduce the liquorrhea, tissue, vascular and pyoinflammatory complications.
References
- Okie S (2005) Traumatic brain injury in the war zone. N Engl J Med 352: 2043-2047. [crossref]
- Battle injuries of skull and brain/ B.V.Gaidar, U.A.Shulev, U.V.Dikarev// Practical neurosurgery: guidelines for doctors; under red. B.V.Gaidar � ???.:?????????, 2002. � P.112-136.
- Gean AD (2014) Brain injury: applications from war and terrorism/ A.D.Gean.- Philadelphia: Lippincott Williams & Wilkins : 338p.
- Besenski N, Jadro-Santel D, Jelavić-Koić F, Pavić D, Mikulić D, et al. (1995) CT analysis of missile head injury. Neuroradiology 37: 207-211. [crossref]
- Clinical practice guidelines (2012) Joint theater trauma system: practical emergency information for critical trauma care from military experts/ United States Army, Depertment of Defense, Medical Research and Material Command, United States Military, United States Army Institute of Surgical Research.
- Clinical guidelines of traumatic brain injury under red. A.N.Konovalov, L.B.Lichtermann, A.A.Potapov. Chapter 21. Battle injuries of skull and brain. M.: 2001. P. 451-474.